By D Kenton Henry, Editor, Agent, Broker 05 May 2026
2027 ACA Health Insurance Changes: What You Need to Know Now (Before It Costs You Later)
If you’re currently enrolled in—or considering—an ACA-compliant individual or family health insurance plan, it’s time to start paying attention to what’s coming.
Beginning in 2027, proposed changes to the Affordable Care Act marketplace could significantly reshape how plans are designed, what they cost, and how easy they are to compare.
Translation: What feels familiar today may look very different in just a couple of years.
1. What “Standardized Plans” Mean (And Why Losing Them Matters)
Most people recognize the Bronze, Silver, Gold, and Platinum categories.
What those levels mean:
They describe how costs are shared:
Bronze → Lower premiums, higher out-of-pocket
Silver → Moderate balance
Gold → Higher premiums, lower out-of-pocket
Platinum → Highest premiums, lowest out-of-pocket
What “standardized” means (this is the key):
Standardized plans require insurers to structure benefits similarly within a level.
That means:
Same or very similar deductibles
Predictable copays
Easier side-by-side comparison
👉 You’re comparing companies, not trying to decode completely different plan designs.
What happens if standardized plans go away?
Every carrier can design plans differently
Two “Silver” plans could behave very differently
Lower premiums may hide higher real-world costs
👉 Bottom line: Comparison becomes harder—and mistakes become more expensive.
2. What “Extended Catastrophic Plans” Actually Means
This is one of the most misunderstood changes.
Today:
Catastrophic plans are:
High deductible
Low premium
Primarily for worst-case scenarios
Evaluated year-by-year
Proposed change: “Extended” catastrophic plans (up to 10 years)
Let’s be very clear:
It does NOT mean:
Premiums are locked for 10 years ❌
Out-of-pocket maximums are fixed for 10 years ❌
It likely DOES mean:
These types of plans can exist as a longer-term coverage option
You may remain in that structure longer without major redesign
They become a more permanent part of the marketplace
By D. Kenton Henry – editor, agent, broker 12 March 2026
Good news for Indiana Medicare Supplement policyholders.
A recent update to Indiana’s new Medicare Supplement Birthday Rule has expanded the period during which eligible individuals may change their Medigap coverage without medical underwriting.
This change may reopen opportunities for some individuals who believed they had already missed their window.
HOT OFF THE PRESS
What Changed?
Beginning March 15, 2026, the Birthday Rule now allows policyholders to apply for a replacement Medicare Supplement policy during a period that begins:
31 days before their birthday and continues through 31 days after their birthday.
This creates a 63-day annual window centered around a person’s birthday.
What This Means
If you currently have a Medicare Supplement (Medigap) policy, you may now apply during this window to switch to the same plan letter offered by a different insurance company.
The insurance company must approve the application regardless of health conditions, provided the rule’s requirements are met.
Example
If your birthday is March 4, your Birthday Rule window would run from approximately:
February 1 through April 4
This means individuals with March birthdays who thought they missed the opportunity earlier this year may still qualify to apply.
Important Requirements
To use Indiana’s Birthday Rule:
• You must currently have a Medicare Supplement policy • The new policy must be the same plan letter as your current coverage • The application must be submitted within the 31 days before or after your birthday • The new policy will take effect on the first day of the month following the application date
Your broker will also need documentation confirming your current plan letter.
Why This Matters
For many seniors, this rule creates an opportunity to:
— without answering health questions or risking denial of coverage.
Need Help Reviewing Your Options?
If your birthday falls within this window and you would like to see whether switching carriers might benefit you, I would be happy to help review your options.
D. Kenton Henry Office: 281-3676565 Text my cell 24/7 @713-907-7984 Email: Allplanhealthinsurance.com
a New Opportunity to Change Your Medicare Supplement Plan Without Health Questions
By D. Kenton Henry – editor, agent, broker
Dear Hoosier Clients and Friends,
Beginning January 1 of this year, Indiana implemented a new consumer protection commonly called the Medicare Supplement Birthday Rule. This new law provides Medicare beneficiaries with an important opportunity each year to change their Medicare Supplement (Medigap) plan without medical underwriting.
For many people, this means you may now be able to replace your current Medicare Supplement policy with a similar or lower-benefit plan and be guaranteed acceptance, regardless of health conditions.
What the Indiana Birthday Rule Allows
Under the new rule, eligible Indiana residents may apply for a replacement Medicare Supplement policy each year around their birthday, and the insurance company must approve the application if the required conditions are met.
This protection is intended to give policyholders a way to review and potentially reduce premiums while maintaining Medicare Supplement coverage.
Key Requirements to Qualify
To take advantage of Indiana’s Birthday Rule, the following conditions must be met:
1. You Must Currently Have a Medicare Supplement Policy
The rule applies only to individuals who are already enrolled in a Medicare Supplement (Medigap) plan.
2. You Must Be Replacing Your Plan With the Same or Lower Benefits
You may switch to another Medicare Supplement plan that offers equal or lesser benefits than your current policy. For example:
Plan G → another company’s Plan G
Plan G → Plan N
Plan F → Plan G
However, you cannot move to a plan with richer benefits under the Birthday Rule.
3. You Must Apply at Least 60 Days Before Your Birthday
Under Indiana’s new rule, the application signed and received date must be within 60 days from the applicant’s birthday. And the effective date must be on the first day of the month that is at least thirty (30) days after the signature date.
The replacement policy will become effective on the first day of your birthday month.
Medical Underwriting Is Waived
If the above conditions are met, the insurance company cannot deny your application due to health conditions.
Why This Rule Matters
Before this rule took effect, Medicare Supplement policyholders often had to undergo medical underwriting to change plans. That meant individuals with health conditions could be:
Declined for coverage
Charged higher premiums
Unable to change carriers
The Birthday Rule now provides an annual opportunity to review your coverage and potentially reduce premiums without having to answer health questions.
Should You Review Your Plan?
Even if you are satisfied with your current Medicare Supplement coverage, it may still be worthwhile to review your options. Insurance companies frequently adjust their pricing, and another carrier may offer the same plan benefits at a lower monthly premium.
The Birthday Rule allows you to explore those options without risking your coverage.
I Am Here to Help
If your current agent has not informed you of this opportunity, ask yourself, “Why?”
If your birthday is approaching and you would like to review your Medicare Supplement options under Indiana’s new Birthday Rule, please contact our office. I can help determine whether changing plans could benefit you.
Thank you for allowing me to continue assisting you with your Medicare coverage.
Sincerely,
D. Kenton Henry Office: 281.367.6565 Text my cell 24/7 @ 713.907.7984 Email: Allplanhealthinsurance.com@gmail.com Https://HealthandMedicareInsurance.com
(What Consumers Need to Know for the 2026 Marketplace)
D. Kenton Henry – editor, agent, broker
As we approach the 2026 plan year, one of the biggest questions in individual and family health insurance is what will happen to Advance Premium Tax Credits (APTCs)—the subsidies that lower monthly premiums for millions of Marketplace enrollees.
Why This Is Happening
During the COVID era, Congress passed temporary legislation — most recently extended under the Inflation Reduction Act (IRA) — which made Marketplace subsidies more generous and available to more households. These enhanced subsidies are scheduled to expire at the end of 2025, unless Congress acts to extend them.
If they expire, the Marketplace will revert to pre-COVID subsidy rules, which means:
1. Lower income thresholds for subsidy eligibility
Some households who qualified for subsidies under the temporary rules will no longer qualify at all.
2. Smaller subsidies for many who remain eligible
People who received very large subsidies during 2021–2025 would see higher net premiums for 2026, even if their income has not changed.
3. The return of the “subsidy cliff”
Under pre-COVID rules, households with income even slightly above 400% of the Federal Poverty Level received no subsidy. The COVID-era rules removed that cliff. If not renewed, the cliff returns.
This is why some people are seeing early projections showing their 2026 premiums rising sharply.
Where Things Stand in Congress
Both parties publicly acknowledge that the expiration would lead to large premium increases for many families. As of today:
There is broad interest in finding a solution, but
No final legislation has been passed,
No guarantee exists that the enhanced subsidies will continue, and
Any resolution will likely be tied to larger budget negotiations.
In short: Congress is still debating it, and the outcome directly affects what consumers will pay for Marketplace coverage in 2026.
What Consumers Should Expect
Until Congress acts, the Marketplace must begin preparing 2026 rates under the assumption that the enhanced subsidies expire. This means:
Preliminary quotes may show dramatically higher net premiums
Some currently subsidized families may temporarily appear ineligible for assistance
Final 2026 subsidy amounts cannot be known until legislation is passed — if it is passed
It is important to remember that this may change, depending on Congressional action in the coming months.
Practical Guidance for Individuals and Families
Don’t panic if early projections show large increases.
Stay informed — subsidy rules may be extended or modified.
Review your 2026 options with a licensed, experienced broker who can calculate subsidies under both scenarios.
Update income estimates accurately during Open Enrollment; small changes can affect substantial tax credit differences.
Bottom Line
The enhanced ACA subsidies that helped make Marketplace coverage more affordable since 2021 are set to expire after 2025, and Congress has not yet determined whether they will be renewed. Until a resolution is reached, 2026 Marketplace premiums may appear significantly higher for many Americans.
I will continue to monitor developments closely and provide updates as soon as new information becomes available.
Additionally—
It has come to my attention that my clients have been told the First Health PPO network plan is being mistakenly interpreted by them as being an Affordable Care Act (ACA) compliant PPO network. As such, they incorrectly believe any and all of their pre-existing health conditions will be covered and that all preventive exams and medicine will be covered at no out-of-pocket cost to them. This is wrong and here is the truth, as confirmed by me and ChatGPT:
✅ 1. There are no ACA-compliant PPO plans available in Texas individual/family (On- or Off-Exchange)
Texas has not had a true ACA-compliant individual market PPO option for several years. All carriers (BCBSTX, Ambetter, United/Optum, Aetna CVS, Oscar, Cigna, Moda, etc.) offer only:
EPOs
HMOs
These networks limit out-of-network benefits and require referrals or tighter network management.
A PPO requires:
National or multi-state contracted provider access
True out-of-network benefits
No referral requirement
No carrier has offered this in the ACA individual Texas market since around 2017–2018.
✅ 2. Aetna is not selling ACA individual/family plans in Texas for 2026 (and has already exited)
Your clients may be confused because Aetna offers:
Medicare Advantage PPOs
Employer-based PPOs
First Health networks tied to group/other products
But Aetna does NOT offer ACA individual/family plans in Texas for 2026.
So if someone believes they have an “Aetna PPO” under an ACA plan, they are mistaken. It is either not an ACA plan, or they are misinterpreting the network type.
✅ 3. If their plan is marketed as “PPO-like,” it is almost certainly:
a) A short-term medical plan
These frequently use PPO networks—including Aetna’s First Health—but they are:
NOT ACA-compliant
Do NOT cover pre-existing conditions
Can cap benefits
Can deny claims based on underwriting
b) A health-sharing ministry
Often marketed as “PPO plans” because they use rented networks, but also:
Not insurance
Not regulated as insurance
No claim guarantees
No ACA protections
c) A fixed-benefit plan that uses First Health or MultiPlan PPO
Again:
Not insurance
No ACA protections
No out-of-pocket maximums
No guaranteed coverage
d) A direct primary care + medical indemnity bundle
These are sometimes misrepresented as “PPO plans,” but they are not.
✅ 4. How to confirm instantly whether the client is on ACA-compliant coverage
Ask for one of the following:
A) The name of the carrier.
If it’s not:
BCBSTX
Cigna
Ambetter
UnitedHealthcare (UHC Marketplace)
Aetna CVS (in some states, but NOT Texas 2026)
Moda
Oscar (until exit)
…then it’s almost certainly not ACA-compliant.
B) A copy of the Summary of Benefits & Coverage (SBC).
All ACA plans must include an SBC — short-term plans and sharing ministries do not.
C) Their monthly bill or ID card.
If it says things like:
First Health Network
MultiPlan PPO
PHCS PPO
Aetna PPO
United Healthcare Choice/Choice Plus PPO
…that is almost certainly a non-ACA plan.
✅ 5. Bottom line for you:
If you believe you they are on an ACA-compliant “Aetna PPO” for individual/family coverage:
You are not. No such product exists in the Texas ACA market. You are almost certainly on a short-term plan, health-sharing product, or fixed-benefit plan using a rented PPO network.
This is an excellent opportunity for ne to help you transition to true ACA coverage, where you will regain:
Pre-existing condition protection
Essential health benefits
No annual/lifetime caps
And – perhaps most importantly – Out-of-pocket maximum protection
Please feel free to call me with any questions you may have or for assistance in obtaining 2026 ACA compliant health insurance. I will make the quoting and application process go as quickly and smoothly as possible whether you quailify for a subsidy or not.
The Open Enrollment Period for a January 1 effective date ends December 15th. You have until January 15th to obtain an effective date of February 1.
D. Kenton Henry Office: 281-367-6565 Text my cell 24/7@ 713-907-7984 Email: Allplanhealthinsurance.com@gmail.com
D. Kenton Henry Editor, agent, broker 30 SEPTEMBER 2025
Medicare 2026: Welcome clients and prospective clients! Before reading this (if you have not already), you should go to your mail box and retrieve your 2026 Annual Notice of Change from Medicare. You were due to receive it no later than today per Center For Medicare Rules and Regulations. If will give you a good idea if you need to re-shop your Medicare Advantage or Part D Drug plan for the coming calendar year. If not, the following changes may.
10 changes to review before the Annual Election period, often referred to as the Open Enrollment (Oct 15–Dec 7)
If you’re on Medicare, 2026 brings important updates—especially to prescription drug coverage. The Part D out-of-pocket cap rises to $2,100, the standard deductible becomes $615, and Medicare’s first negotiated drug prices start on January 1, 2026. Medicare Advantage also gets new guardrails around prior authorization and appeals, and some supplemental “perks” are being narrowed. Check your Annual Notice of Change (ANOC) (it should arrive by Sept 30) and compare your plan options—small differences can mean big savings. If you’d like help, I’ll review your medications, doctors, and benefits to make sure you’re in the right fit for January 1.
Here is an itemized list of the 10 Key Changes:
Medicare changes your 2026 plan review should cover
1) Part D’s annual out-of-pocket cap rises to $2,100. Once a member’s 2026 Part D out-of-pocket spending reaches $2,100, they’ll pay $0 for covered Part D drugs for the rest of the calendar year.
2) The standard Part D deductible increases to $615. Plans can’t set a deductible higher than $615 in 2026 under the redesigned Part D rules.
3) Drug price negotiations start showing up at the counter. Medicare’s first set of negotiated Maximum Fair Prices (MFPs) for 10 widely used Part D drugs take effect January 1, 2026. Members should review their ANOC and plan formularies to determine how these prices impact their medications.
4) Insulin and adult vaccines: protections continue. Part D insulin remains capped and no-deductible; starting in 2026, the cap is the lesser of $35, 25% of the MFP, or 25% of the negotiated price. ACIP-recommended adult vaccines remain $0 under Part D.
5) “Pay-over-time” for prescriptions auto-renews. The Medicare Prescription Payment Plan (monthly billing instead of paying large amounts at the pharmacy) auto-renews in 2026 unless the member opts out. It smooths payments but doesn’t lower total costs—good to remind clients who tried it in 2025.
6) Medicare Advantage prior-auth and appeals guardrails tighten. For 2026, CMS says MA plans must honor previously approved inpatient admissions (can only reopen for obvious error or fraud), and CMS closes appeals loopholes so members and providers receive required notices and can appeal adverse coverage decisions. Expect fewer mid-stay reversals. Centers for Medicare & Medicaid Services
7) Limits on certain “extra perks” in MA (SSBCI) take effect. CMS codified non-allowable Special Supplemental Benefits for the Chronically Ill—examples include non-healthy food, alcohol, tobacco, and life insurance. Some plans may rebalance extras as a result.
8) Star Ratings update: new/returning measures. 2026 Stars add or reintroduce measures like Kidney Health Evaluation for Patients with Diabetes plus Improving/Maintaining Physical and Mental Health (weight = 1). Tougher cut points in 2026 may shift plan bonuses and benefit richness—worth watching locally.
9) Part D benefit design shifts behind the scenes. Liability shares change across phases (plans, manufacturers, CMS), and there’s a new subsidy for selected (negotiated) drugs. Members may see formulary/tier adjustments—another reason to compare plans.
10) ANOC timing: what to tell clients. Remind everyone: Annual Notice of Change (ANOC) letters arrive by September 30 each year; if they didn’t see one, call the plan. Open Enrollment runs Oct 15 – Dec 7 for Jan 1 effective dates.
Check your Annual Notice of Change (ANOC) (it should arrive by Sept 30) and compare your plan options—small differences can mean big savings. If you’d like help, I’ll review your medications, doctors, and benefits to make sure you’re in the right fit for January 1.
Other Developments
Some Medicare Advantage supplemental benefits (i.e. nutrition support, OTC medicine) may be reduced in favor of core services.
In six states, prior authorizations for certain Original Medicare services will be tested.
Part B and Part D premiums and deductibles are both set to increase—Part B premium up ~11.6%, and Part D premium by about 6%.
Who Am I?
In addition to being the editor of this blog I have has been helping individuals and families navigate the health and Medicare insurance landscape since 1986. With nearly four decades of experience, he specializes in Medicare Supplement, Medicare Advantage, and Medicare Part D prescription drug plans.
As an independent broker, I am appointed with virtually every competitive, A-rated Medicare insurance company in Texas, Indiana, Ohio, and Michigan. This broad access allows him to recommend the plan that truly best fits each client’s needs.
Above all, I work for my clients—not the insurance companies. You will never pay more by enrolling through me than you would if you purchased an insurance product directly from the carrier. My mission is to provide clear guidance, personalized recommendations, and ongoing support to ensure my clients get the coverage and peace of mind they deserve.
If you have any questions about 2026 Medicare Part D prescription drug plans, Medicare Advantage, or Medicare Supplement (Medi-Gap) policies, please give me a call.
Average premiums, benefits and plan choices for Medicare Advantage and the Medicare Part D prescription drug program should remain relatively stable next year, CMS said in a Sept. 26 news release. But MA enrollment is projected to decrease 900,000 in 2026.
Despite a slight dip in available MA plans nationally, over 99% of Medicare beneficiaries will still be able to access an MA plan.
The agency estimates the premiums for MA plans to drop from $16.40 to $14.00. On average, the total premium for standalone Part D is estimated to fall $3.81. CMS’ July forecast predicted elevated Medicare Part D base premium increases in the neighborhood of 6%.
Finding Your Doctor and Understanding Subsidies in HMO Plans
Shopping for individual or family health insurance can feel like navigating a maze—with dead ends, confusing signs, and few clear answers. Two of the most common pain points for shoppers are (1) trying to keep your current doctor while limited to an HMO network and (2) figuring out whether you qualify for a subsidy, known as an advance premium tax credit (APTC). Both challenges can make the process frustrating and overwhelming, especially during open enrollment when time is limited.
The HMO Headache: “Will My Doctor Be Covered?”
One of the biggest shocks people face when shopping for health insurance is realizing that their trusted doctor or medical provider might not be covered under a new plan—especially if it’s an HMO (Health Maintenance Organization). Unlike PPOs (Preferred Provider Organizations), which offer broader provider access and out-of-network options, HMO plans restrict coverage to a specific network of doctors and hospitals. If your doctor isn’t in the network, you may have to pay the full cost of your visit out of pocket—or switch doctors entirely.
Unfortunately, trying to find this information is often easier said than done.
Outdated or Inaccurate Provider Directories: Online directories can be incomplete or outdated. It’s not uncommon for a provider to be listed as “in-network” only for you to find out later they’ve left the plan.
Hard-to-Navigate Insurance Websites: Many insurance carrier sites don’t make it easy to search by doctor name, location, or specialty. Even worse, each plan may have its own “network tier,” adding another layer of complexity.
No Universal Search: There’s no centralized tool that lets you enter your doctor’s name and see every marketplace plan that includes them. You have to check each insurance company or plan individually.
For people with ongoing care needs—like managing chronic conditions or continuing with a trusted pediatrician or specialist—the possibility of switching providers isn’t just inconvenient, it can feel risky.
The Subsidy Puzzle: “Do I Qualify for Help Paying My Premium?”
The Affordable Care Act (ACA) made health insurance more accessible by offering subsidies for people who meet certain income guidelines. These subsidies, officially called advance premium tax credits, lower your monthly premium based on your household size and income.
The good news is that many people qualify.
The bad news is that determining whether you qualify can feel like filling out a tax return just to get a quote.
Income Guesswork: Subsidy eligibility is based on your estimated household income for the upcoming year. That’s right—you must predict your future income, even if you’re self-employed or work variable hours.
Family Dynamics Matter: Your household size includes dependents—even if they don’t need insurance—and income from every working member. This means getting it right often requires gathering data from multiple people.
Mid-Year Changes Complicate Things: If your income or family size changes mid-year, you may need to report it or risk having to repay part of your subsidy at tax time.
The ACA “Cliff” and “Glide Path”: Previously, you could lose your subsidy entirely if your income was even $1 over the limit. Recent changes have smoothed this out, but they are still complicated and frequently misunderstood.
And while tools like Healthcare.gov’s calculator are helpful, they often rely on broad estimates. They can’t account for all variables, such as gig work, investment income, or multiple part-time jobs.
Why It Feels So Frustrating
When you shop for health insurance, you’re not just picking a product—you’re making decisions that affect your finances, your family’s well-being, and your access to care. The stakes are high, yet the process often feels opaque and unnecessarily complicated.
You’re expected to:
Compare dozens of plans with unfamiliar terms,
Check if your providers are covered (without reliable tools),
Predict your income a year in advance,
And hope you don’t make a mistake that costs you money or coverage.
Tips for a Smoother Experience
While the system isn’t perfect, there are ways to reduce frustration:
Use a Licensed Agent or Broker: Agents specializing in ACA plans can often help you find plans that include your provider and determine if you qualify for subsidies—all at no extra cost.
Call Your Doctor’s Office: Don’t rely solely on insurance directories. Call your provider’s office directly to confirm if they accept a specific plan.
Keep Documentation: If your income fluctuates, keep clear records. This will help you provide accurate estimates and support your case in the event of an audit or dispute.
Update Changes Promptly: If your income or household size changes mid-year, report it on your health insurance marketplace to avoid surprise bills or tax penalties.
In Summary
Shopping for individual or family health insurance can be a stressful process—especially when you’re trying to keep your doctor and figure out if you qualify for financial help. Between restrictive HMO networks and confusing subsidy rules, it’s easy to feel stuck. But with a little extra diligence, some expert help, and the right questions, you can find a plan that fits your needs without sacrificing peace of mind.
If the process still feels overwhelming, you’re not alone. Many Americans share the same frustrations—and continue to hope for a more user-friendly system in the future.
Below is a chart outlining estimated income thresholds for qualifying for an Advance Premium Tax Credit (APTC) in 2025. These thresholds are based on a percentage of the Federal Poverty Level (FPL), which is adjusted annually. For simplicity, the chart includes 2024 FPL figures (used for 2025 coverage) and the income ranges (100%–400%+ of FPL) where most people qualify for subsidies under the ACA.
📝 Note: Due to the American Rescue Plan and Inflation Reduction Act, subsidies may extend beyond 400% of the FPL, with a sliding scale that caps the percentage of income spent on premiums. These extended subsidies are currently in place through 2025.
2024 Federal Poverty Level (FPL) and APTC Income Guidelines for 2025 Coverage
Household Size100% / FPL400% / FPLTypical APTC Eligibility Range
Minimum Income: You must earn at least 100% of the FPL to qualify for a subsidy in most states. In Medicaid expansion states, if you earn less than 138% FPL, you may qualify for Medicaid instead.
Upper Limit Removed: Thanks to temporary reforms, people earning above 400% FPL may still qualify for a subsidy if the cost of the benchmark plan exceeds ~8.5% of their income.
Household Size: Includes you, your spouse, and any dependents claimed on your tax return.
💡 What This Means for You
If your estimated annual income falls between the ranges shown above, you likely qualify for help paying your monthly health insurance premium.
Households earning more than 400% of the FPL may still qualify if their premiums exceed about 8.5% of income, thanks to current federal subsidy expansions.
Eligibility is based on your tax household — including you, your spouse, and dependents you claim on your tax return.
If your income is below 138% FPL, you may qualify for Medicaid (in most states).
DO NOT CALL AN 800 NUMBER and talk to some anonymous employee of an insurance company. Not only are they restricted to limiting you exclusively to their company’s options—but your personal information will be instantly sold and shared. Your phone is going to begin ringing off the hook!
I’ve been specializing in Medicare-related insurance for over thirty years, right here in The Woodlands, Texas, USA! I represent every Medicare-related product, including Supplement, Advantage, and Part D Drug plans, from virtually every “A” rated company doing Medicare-related business in Texas. And I CHARGE NO FEE for my services! Deal with a local agent/broker who values your business enough not to share it with anyone!
D. Kenton Henry Editor, Agent, Broker Office: 281.367.6565 Text my cell 24/7 @713.907.7984 Email: Allplanhealthinsurance.com@gmail.com
By D. Kenton Henry Editor, HealthandMedicareRelatedInsurance.com Agent, Broker 28 January 2025
Hello again, and welcome to 2025! Early last October, just prior to the Medicare Annual Election Period (AE), I informed you of the many changes coming to Medicare Part D Prescription Drug Plans in the coming calendar year in which we now find ourselves. I explained the pros and cons that many of you are now experiencing in real time. On the positive side, I am certain many are celebrating that their annual drug costs (for Part D covered drugs) can never go beyond the new annual maximum out-of-pocket (OOP) of $2,000! And, hopefully, you are not experiencing the negatives—such as learning your Rx drug (which was previously covered) is no longer or its price has increased dramatically! Once again, we realize the government can giveth or taketh away.
But there is one thing in which you have a certain amount of control, and this is the ideal time of year to exercise that control. During the AEP, insurance companies, agents, and brokers work overtime seven days a week to see that their clients, and prospective clients, are guided to the Medicare Advantage and Part D Drug plans that best meet their needs. To do this correctly, an agent must understand the client’s needs and objectives and then do, what is often, extensive research to ensure a person’s drugsare covered and they have access to their preferred providers. In some cases, this can take minutes and, in others, hours over repeated phone calls. In most cases, you won’t get the latter from a company employee on the end of an 800 number, but you will get it from me.
Now that the AEP ended December 7th, agents have much more time to assist you in improving the cost of your Medicare Supplement coverage. As you may know, Medicare Supplement is not subject to annual enrollment periods in Texas or most states. What this means, is you can re-shop your Supplement coverage to find identical (or improved) coverage 365 days per year. The incentive for doing so is that you may save 30% or more in premiums. Because Medicare Supplement premiums go up each year as we age, it doesn’t take too many years before most of us begin to wonder if our premium is still reasonable or competitive. The reality is, if your policy is three years or older, you will indeed safe significantly by switching to a policy with the same letter designation, e.g., Plan G. I have many clients whose policy premiums had increased to well over $300 per month that I was able to lower (with new coverage) to less than $200 per month!
Additional reasons to re-shop now are that a few “A” rated companies are particularly interested in expanding their block of business. This does not imply a compromise in the quality of their customer service or rate stability. It simply means that through prudent management and staff expansion, they can be more competitive, significantly lowering your premium. Additionally, you may now have a spouse, or in some cases, simply another adult living with you—making your new policy available for a “Household Discount”. Typically, these discounts can lower your premium 7-12%, and—if the other person is covered by the same company—that discount will apply to their existing policy also!
So what is the catch? The catch is that now that you have been in Medicare Part B 6 months or more, you must go through underwriting and be approved for the new coverage based on your current health and relatively recent health history. The bottom line is, if your current conditions are well controlled with medication, you do not suffer from any chronic condition that poses a long-term liability to the insurance company, and you have no pending surgeries or hospitalizations—you are a good candidate for replacement coverage. The worst scenario is you are declined. In this case, all you are out of is the small amount of time you took to complete the application.
THE FOLLOWING IS A SYNOPSIS OF THE PROS AND CONS OF RE-SHOPPING YOUR COVERAGE:
Re-shopping a Medicare Supplement (Medigap) policy can provide several advantages for recipients, especially if their needs or circumstances have changed since they first enrolled. Here are the key benefits:
1. Cost Savings
Premium Reduction: Medigap premiums can vary significantly between providers for the same coverage. Shopping around may uncover lower premiums for the same plan (e.g., Plan G or Plan N).
Health Status Discounts: If your health has improved since your initial enrollment, you might qualify for a lower premium rate with another insurer.
Household Discounts: Some insurers offer discounts if multiple members of the household enroll in their Medigap plans.
2. Better Coverage Options
Change in Needs: If your healthcare needs have increased or decreased, you might find a plan that better aligns with your current situation, such as switching from a high-deductible plan to one with lower out-of-pocket costs.
Additional Benefits: New Medigap plans might include perks like fitness programs, telehealth, or wellness benefits that weren’t available when you initially enrolled.
3. Access to New Insurers
Competitive Market: New insurers entering the market may offer attractive rates or better customer service than your current provider.
Provider Reputation: Switching to a more reputable insurer can improve your overall satisfaction and ensure reliable claims processing.
4. Avoiding Rate Increases
Age-Based Increases: Some policies increase rates as you age. Shopping around may allow you to switch to a community-rated policy where premiums are based on a group average rather than individual age.
Annual Adjustments: If your current insurer has raised premiums significantly, exploring alternatives can help you lock in a more stable rate.
5. Improved Customer Service
If your current insurer has poor customer service or limited support, switching to a provider with higher satisfaction ratings can enhance your overall experience.
6. Medicare Advantage Comparison
While re-shopping Medigap policies, some recipients may realize that a Medicare Advantage (Part C) plan is more cost-effective or suitable for their needs. These plans often include additional benefits like dental, vision, and hearing coverage.
7. Regulatory Benefits
Guaranteed Issue Rights: In some situations (e.g., losing coverage or moving), recipients have guaranteed issue rights, allowing them to switch Medigap plans without medical underwriting.
Trial Rights: If you tried a Medicare Advantage plan for less than 12 months and decide to switch back to Original Medicare, you may have a guaranteed right to re-enroll in a Medigap plan.
8. Customizing for Future Needs
Planning ahead for potential healthcare changes can ensure that you are prepared for costs that might arise later, such as skilled nursing care or extensive outpatient services.
Considerations When Re-Shopping
Medical Underwriting: Outside of guaranteed issue periods, you may need to answer health questions, which could affect your eligibility or rates.
Plan Standardization: All Medigap plans with the same letter (e.g., Plan G) offer identical core benefits, regardless of the insurer, making it easier to compare prices.
Timing: The best time to switch is typically during your open enrollment period or when you have guaranteed issue rights.
By re-shopping their Medigap policy, Medicare recipients can ensure they are getting the best value and coverage for their evolving needs.
I am an independent agent with more than three decades in the medical insurance industry. As I have aged, so have my clients, and Medicare-related insurance (Supplement, Advantage, Part D) has become my specialty. I represent virtually every “A” rated insurance company in Texas as well as three others. I provide objective advice based on empirical numbers inclusive of costs and satisfaction surveys.
Significantly, I do not charge a fee for my service. You are charged no more for acquiring a product through me than if you went in the front door of the insurance company whose product you elected and acquired it directly from them!
Please allow me to assist you in lowering the cost of your Medicare-related insurance. I look forward to working with you!
By D. Kenton Henry Editor, Agent, Broker HealthandMedicareInsurance.com 11 September 2024
Welcome, fellow boomers and others blessed to have lived long enough to find yourself here. I believe you recognize that the information in my blog posts can contribute to this leg of our journey being the longest and most rewarding. I’m right here with you and doing my best to make it so for all of us. Coming changes in 2025 Medicare plans are significant, so please read this and feel free to take notes. They could impact you and probably will.
We will begin with what your Medicare Part B premium to Medicare for Out-Patient Care will go to: For those earning less than $105,000 your premium will go to $185.00 (up from $174.70) For those in the highest income bracket, earning greater than $500,000 your premium will go to $628.90 (from $594.00) For every income block in between, couples filing jointly, and what Part D premiums to Medicare will go to, please click on this link and scroll down: https://www.irmaacertifiedplanner.com/2025-irmaa-brackets/
An Annual Notice of Change (AOC) from your Medicare Part D prescription drug plan or a private insurer’s Medicare Advantage plan is due you. It will arrive in the United States mail and, per Medicare rules, by September 30th. So, like the pretty woman in the image above, open it and read it. It outlines how much your premiums, deductibles, and co-pays will differ in the coming year. Will your drugs be covered, and will your current drug plan even be available? We don’t yet know. Mutual of Omaha notified agents and brokers that it is withdrawing altogether from the Part Drug plan market beginning January 1. If you are currently with them or have any other plan that is exiting the marketplace, follow the instructions in the next paragraph.
According to eHealth, a mere 36% of those surveyed claim the AOC to be “readily understandable.” The author of the attached article recommends you spend at least 30 minutes reviewing it. However, if you finish this article, you can cut that time considerably. If you have finished all and still feel you are among the remaining (up to) 64%—please call me @ 281-367-6565.
This article is a follow-up to my last blog post on September 3rd. “MAJOR CHANGES IN MEDICARE PART D DRUG PLANS ARE COMING OUR WAY (what we know. and one thing we don’t know).” To read it, please click on this link. (if necessary, copy and paste it in your browser’s URLbox and hit enter):
Well, now we know more of the potential compromises mentioned or alluded to in that article. All of these are covered in detail in Feature Article 1 below.
The changes addressed here are largely because of the new $2,000 per year limit on Medicare Part D drug costs in 2025 (versus $8,000, plus 5% thereafter, in 2024). That leaves Medicare Part D insurance companies looking for ways to compensate for the additional costs shifting from you to them. Come January, you will meet a new deductible of up to $590 (from $545) for applicable drugs. Typically, your plan will apply this to brand-name drugs and not Tier 1 or Tier 2 generics.
Beyond that, the Gap, commonly referred to as the “donut hole” (in which you were previously responsible for 25% of your drug costs), has been eliminated entirely. You will have entered the “Initial Coverage” phase in which your elected drug plan will pay 65% of your applicable drug costs, and you will pay 25%. The Manufacturer (pharmaceutical company) will discount the remaining 10%. When you hit your maximum Out-of-Pocket (OOP) threshold of $2,000, you enter “Catastrophic Coverage”. At that point, your plan will pay 60%. Reinsurance (CMS, the Center for Medicare Services, i.e., the government) will pay 20%, and the Manufacturer will pay the remaining 20%. You will pay $0.
This, of course, sounds very well and good! And for those utilizing large quantities of drugs, or expensive drugs, this will indeed be of great benefit. But in what ways may the drug plans “compensate” for the additional costs they will bear? Much of such was referenced or alluded to above. However, please permit me to drill down on potential measures drug plans may take to offset their increased share of your drug cost. *(I am a Medicare Insurance product broker and not a C.P.A. As such, I will not address the impact on the taxpayer of their increased share of Medicare drug costs in this forum. wink. wink 😉
The drill down:
In addition to the higher deductible, higher premiums may be in store. But it could have been a lot worse. CMS did health insurance companies a favor with a “premium-stabilization” plan. In 2025, they will give them a subsidy in exchange for not “slapping members with exorbitant premium hikes. So, “what might have been a 40%, 50%, or higher premium increase may only be as high as 25%. Either way, it will be a sticker shock when some see how their premiums changed.” *(a paraphrase a quote in Feature Article 1)
The Kaiser Family Foundation says the average cost of a stand-alone Part D drug plan is $43. I have seen previews of premiums which will be $0, but others, have risen. In addition to your premium, co-pays for your drugs could go substantially higher. If your drug plan is obligated to charge you less for (or cover more of) a particular drug, are they simply going to charge you more for others?
And what about “Value Added Benefits” (VAB) available in some Medicare Advantage Plans? These include vision, hearing, and dental services. Other examples include acupuncture, bathroom safety devices, and wigs for hair loss. And what about your gym membership? Embedded dental insurance has been dramatically cut back or removed completely.
VAB are not covered by Original Medicare. Medicare Advantage has been able (often along with a $0 premium) to offer these things as an additional incentive to encourage enrollment in their plans. However, because you left Original Medicare and “assigned” the administration of your benefits and claims to the Advantage company when you enrolled, your plan can choose to provide these ancillary benefits that Original Medicare does not. Or they can choose to cover them no longer. This discretion is on their part because the provision of VAB benefits is not codified in law or per CMS regulation. Resultingly, they are not guaranteed. They are optional benefits that the plans have the right to withdraw at any time. I hope you can continue to “workout” at the gym, at your plan’s expense, in 2025 and beyond. But be prepared to purchase a home gym kit if you learn your membership is downgraded or your Advantage plan disappears entirely.
With no obligation, please feel free to contact me for clarification of these relevant issues and additional guidance in navigating the Medicare system and the changes referred to here. I’m in Medicare with you. I am a “Boomer” who has spent the better part of his life in the medical insurance market. For years, I have assisted individuals, families, and businesses in identifying and enrolling in health insurance plans that came as close as I could get them to fully meeting their medical insurance wants and needs.
To sum things up, I work for my clients. I work for you. Not the insurance company. I study, take their tests, and “certify” to represent their products each calendar year. I just completed certifying with approximately 14 companies in preparation for marketing their products in 2025. They do not pay to renew my licenses or my Errors and Omissions insurance, nor do they cover my office insurance and expenses. Neither they, nor anyone else, pay me wages or a salary. And that is great! I knew and understood those terms when I went out on my own. And that is precisely why I did it. I did not want to be beholden to the insurance company.
After becoming independent, the list of companies I was contracted with grew to over 40 during the 1990s. That number has changed as many of those companies went the way of the steam engine with “Obamacare” and all the red tape and regulations that come with it and remaining in the industry. But I persist. I remain positioned to provide you with virtually every available Medicare and health insurance product in your region.
In conclusion:
If you’re reading this, chances are you remember Jim Rockford (a private detective, portrayed by the actor the late James Garner) in his TV show, The Rockford Files (you can hear the opening music now, can’t you?). In the prelude to each episode, you see his cassette recording answering machine and hear the message, “This is Jim Rockford. At the tone, leave a message …”.
Should you get mine, please do the same. Or you may simply text me.
FORTUNE Richard Eisenberg Updated Mon, Aug 26, 2024
Why this year’s Medicare Annual Notice of Change will be vital reading for beneficiaries
In this article:
If you’re on Medicare, you’ll be getting one or two Annual Notice of Change letters in your mail or email this September about your 2025 coverage and costs. You may be tempted to ignore what looks like junk, as nearly a third of recipients do, according to an eHealth survey.
Don’t.
“So often, a person who is quite happy with their plan and doesn’t bother to look at their Annual Notice of Change then gets a nasty surprise in January” when the plan’s new costs and coverage kick in, says Danielle Roberts, author of 10 Costly Medicare Mistakes You Can’t Afford to Make and founding partner of Boomer Benefits, which sells Medicare policies.
What is an Annual Notice of Change?
An Annual Notice of Change from your Medicare Part D prescription drug plan or a private insurer’s Medicare Advantage plan lays out how much your premiums, deductibles, and co-pays will differ in the year ahead and whether the plan will even be offered. (Medigap plans don’t send these notices because they don’t change much year to year.)
An Annual Notice of Change from your Part D plan also says whether your prescriptions will be covered and, if so, how much you’ll pay. A Medicare Advantage Notice of Change will tell you if your doctors and hospitals will remain in the plan’s network.
While this information is always essential to make smart choices during Medicare’s eight-week open enrollment period (Oct. 15 – Dec. 7), experts say reading your Annual Notice of Change is especially important in 2024.
“There is an excellent chance that something is changing on your plan,” says Roberts. “This year, more than ever, we can expect big changes in the plans.”
Surprising effect of the $2,000 prescription drug cap
That’s largely due to a major Medicare change coming in 2025: the new $2,000 cap on out-of-pocket costs for prescriptions covered by a Part D plan.
Since Part D health insurers will be on the hook for more prescription costs due to the cap, they’ll be looking for ways to compensate.
That could mean higher premiums (currently $43 a month for stand-alone plans, on average, according to KFF), deductibles, and co-pays—possibly substantially higher than in 2024.
“I have been very, very concerned about what the $2,000 cap was going to do to Part D premiums,” says Roberts.
The prescription drug change in 2025 could also lead to your Part D plan no longer covering certain medications you take or raising prices of ones it will.
Medicare Advantage plans—some facing profit squeezes currently—often include Part D coverage, so they may respond to the $2,000 cap by trimming or eliminating benefits to keep their popular $0 premiums intact, experts expect.
As a result, your Medicare Advantage benefits that original Medicare can’t offer—such as dental, vision, hearing, and gym memberships—could be less attractive than in 2024, or possibly gone entirely.
“It really will be important to understand what’s changing in the coming year in my current plan and does the plan still fit?” says eHealth CEO Fran Soistman. “Does it still provide the value that it did when I elected to go in it in the first place?”
Reading and understanding the Notice of Change
Your Annual Notice of Change will tell you—if you can understand it.
Only 36% of Medicare beneficiaries surveyed by eHealth said their Annual Notice of Change letter is “readily understandable.”
Figure on spending about 30 minutes closely reading your Annual Notice of Change to see exactly what will be different in 2025 and whether you’ll want to switch plans or coverage next year as a result.
During open enrollment, you can switch from your current Part D plan to another, from your Medicare Advantage plan to another, from Medicare Advantage to original Medicare as well as from original Medicare to a Medicare Advantage plan.
But don’t feel compelled to switch plans just because your Annual Notice of Change says your premium will go up a little or a benefit will be trimmed slightly.
“If there’s a modest benefit decrease or premium increase, but they’re satisfied with what the carrier is providing, people shouldn’t make a change,” Soistman says.
However, he added, if a medication you take will no longer be covered or your physician or hospital won’t be in network, that’s an important change that may persuade you to switch coverage.
The Medicare Plan Finder on Medicare’s site will let you compare Part D and Medicare Advantage plans for 2025.
And, as Philip Moeller writes in the forthcoming revised edition of his book, Get What’s Yours for Medicare, if your Medicare Advantage plan won’t include your favorite doctor or hospital in its network in the year ahead, it’s legally obligated to work with you to identify other physicians or hospitals in its network that you’d like.
A new program to help avoid big premium hikes
To help prevent drastic Part D premium increases, the government’s Centers for Medicare and Medicaid Services recently threw a bone to health insurers with a premium-stabilization plan.
Medicare will provide a special subsidy to those insurers for 2025 in exchange for avoiding slapping members with exorbitant premium hikes.
“It should take what might have been a 40%, 50%, or higher premium increase down to probably 25%,” says Soistman. “It’s still going to be a bit of sticker shock when some people see how their premiums changed.”
Roberts says, “I’m still somewhat concerned about premiums, but I feel a little better after the stabilization program announcement.”
Getting help if your Medicare plan will change
After reading your Annual Notice of Change, you may want to get help deciding on the right Medicare plans for 2025 and to understand the implications of coming changes to your plans.
You can ask a Medicare broker or agent for assistance; there’s a directory at the National Association of Benefits and Insurance Professionals site. The sooner you do, the better, since agents and brokers will be swamped near the end of open enrollment.
“At Boomer Benefits, we have to stop taking new requests after Thanksgiving,” says Roberts.
If one of your prescriptions won’t be covered by your Part D plan in 2025, call your doctor to see if another covered medication would be okay or if you should find a new plan that includes it, Roberts advises.
For information about Part D and Medicare Advantage plans without purchase recommendations, try yourState Health Insurance Assistance Program or visit Medicare’s site or call Medicare’s toll-free number.
More time for open enrollment?
Soistman believes all the changes coming to Part D and Medicare Advantage plans for 2025 will push back the arrival of the Annual Notice of Change documents to the last two weeks of September.
If so, this will give people with the plans less time than normal to read the notices before open enrollment.
The eHealth agency has asked the Centers for Medicare and Medicaid Services to extend open enrollment by about five days to give beneficiaries, insurers, and Medicare brokers more time. Boomer Benefits favors the extension, too.
So far, the government hasn’t responded to eHealth’s proposal.
Could the 2025 open enrollment become Medicare’s equivalent of the Department of Education’s FAFSA financial-aid form fiasco of chaos and confusion?
“I don’t think it will be quite as drastic. I think it is going to be a year of change, though,” says Soistman. “And change is hard for people.” ********* Please follow me follow D. Kenton Henry @Https://HealthandMedicareInsurance.com
In addition to owning the first insurance agency in The Woodlands, Texas, and most of the United States, to create a website (Allplaninsurance.com) in 1995, I was among the first to offer Medicare Advantage and Medicare Part D Prescription Drug Plans (MAPD plans) to Medicare recipients following their creation by the Medicare Modernization Act of 2003. Congress created them to provide a lower premium insurance product as an alternative to Medicare Supplement policies, which has been the standard insurance product to serve as secondary insurance covering medical expenses not paid by Original Medicare. And—with premiums as low as $0—they have certainly done that. Contrary to what may be the common perception of the public, every good agent has a little bit of social worker in them and wants to think they have really helped a person and improved their situation. As an agent (before the advent of Medicare Advantage plans), I would sit across coffee tables from prospective clients living in single-wide trailers and subsisting on social security income alone. I would watch tears come in their eyes as they told me they simply did not have another dime to spend on insurance, leaving me to drive off and them no better off for my visit. So, from that standpoint, they have been a source of great relief for me as well as my clients.
In addition to lower premiums, MAPD plans offer other advantages. Specifically, they are:
The convenience of combining medical coverage with prescription drug coverage under the cover of one policy. Effectively eliminating the necessity of paying a second premium for the latter.
The provision of “extra” benefits such as dental, vision, and hearing benefits
“Guaranteed Approval” during the Annual Election Period October 15th and December 7th and the option of changing your plan each January 1 as the plans and your needs change.
Premiums are not age-based and do not increase due to age as one gets older.
Seniors are inundated with seemingly endless television and radio commercials promoting Medicare Advantage plans ad infinitum. But while they drive home the advantages mentioned above, they virtually never mention the disadvantages or compromises that come with electing them over a Medicare Supplement policy. There are many reasons for this, but this is the one most relevant to you:
Medicare, like Social Security, is hemorrhaging dollars. Please don’t take it from me. Google it. Financial prognosticators project it will enter a default position by 2031. Medicare trustees say the Part A (Hospital and Skilled Nursing coverage) program will begin running deficits again in 2025, drawing down the trust fund until it depletes in 2031. After that date, the program will not bring in enough money to fully pay out Part A benefits. *(See Feature Article 2 below.)
Now, we all know our government will just tax us more, and our treasury will print enough more money to keep things going. But the bottom line is that Medicare is seeking any way of saving money and limiting its losses. The easiest way to do this is to lower its share of claims. The easiest way to lower its share of claims is to increase enrollment in Medicare Advantage plans relative to Medicare Supplement. And why is that?
Opposed to Supplement, Advantage plans . . .
1)Force the insured member to share in more expenses as the medical claims come in.
2) They influence the member to utilize a limited network of providers or pay a higher cost for not.
3) They subject the member to preauthorization of medical tests and procedures, often resulting in significant delays in treatment. *(See Feature Article 1, 2 and 3 below.)
4)Advantage plans that combine prescription drug coverage with medical coverage (MAPD plans) lock the member into a drug plan that may not provide the lowest total cost for drugs or cover them in the first place.
5)Once a member foregoes Medicare Supplement in favor of an Advantage plan beyond 12 months, they may find themselves locked into an Advantage plan—and out of a Medicare Supplement plan—due to preexisting medical conditions for the remainder of their lives.
One reason for these differences in how things are covered is that when a person elects Medicare Advantage, their benefits and administration are assigned to the insurance plan and company issuing it and away from Medicare. Medicare no longer plays a role in your coverage. As Advantage plans are allocated a limited amount of dollars per plan member, the companies will seek to limit expenditures. Recent adjustments in budgets for the plans will result in more of this. *(See Feature Articles below.)
And now, we learn that in addition to the increasing number of denials for tests and procedures by Advantage plans, Medicare is allocating less money to cover benefits, resulting in an actual reduction in benefits in 2025. Depending on the Medicare Supplement plan option (A-N) one elects, these compromises seldom, if ever, apply to their coverage.
All this being said, we get back to affordability and the reality that Medicare Supplement premiums will increase due to the member’s age as the member ages. This could bring me back to that coffee table where clients simply can no longer afford their premiums. While their costs for treatment may increase, some will need a lower premium to afford some type of coverage. Those people should know I offer Medicare Advantage plans from virtually every major carrier in one’s county or region. These include (among others) Aetna, Anthem, AARP Unitedhealthcare, BlueCross BlueShield, Cigna, Kelseycare Advantage, and Wellcare.
Regardless of your situation, I offer whatever product is appropriate and best suited to meet your Medicare-related insurance needs. When you work with me, I will be an advocate on your behalf. I represent you over the insurance company. Yes, I still have a little bit of social work in me.
Please get in touch with me. I am waiting to answer your questions and assist you with your coverage.
Hospitals’ Medicare Advantage problem hits an inflection point
Jakob Emerson – 5 April 2024
The tensions between hospitals and Medicare Advantage plans continue to grow. With the program hitting nearly 34 million enrollees in March, paired with recent policy moves by the federal government, the scene has been set for those relations to worsen.
“The relationship between hospitals and managed care is strained at best right now,” Chip Kahn, president and CEO of the Federation of American Hospitals, told Becker’s. “[Insurers] are finding every way to not pay for the care that Medicare beneficiaries should receive. I don’t know how the issue gets worse — we’re at a critical stage, and I think CMS is sending those signals.”
On April 1, CMS finalized a slight decrease in MA benchmark payments for 2025. The agency has also issued more strict prior authorization rules this year and cracked down on when MA plans must cover inpatient care.
The health insurance industry has said the new rates will “put even more pressure on the benefits and premiums” of MA beneficiaries, a warning that individual insurers have also issued in recent months.
“Payers know that they’re going to have to cut supplemental benefits, and premiums may even have to go up, but I wouldn’t want to be the first one to do it,” Scott Ellsworth, founder and president at Ellsworth Consulting, told Becker’s. Mr. Ellsworth is a former insurance executive, overseeing entire divisions at Centene, Optum and a BCBS plan throughout his career.
“Seniors have seen their benefits get better every year, but now we’re at an inflection point and the free lunch is over,” he said. “There is going to be a sharing of the pain. Providers have disproportionately shared the pain and now you’re seeing many of them say ‘enough is enough, we’re out.'”
In 2023, Becker’sreported on at least 15 hospitals and health systems nationwide that dropped some or all of their Medicare Advantage contracts. Among the most commonly cited reasons are excessive prior authorization denial rates and slow payments from insurers. Some systems have noted that most MA carriers have faced allegations of billing fraud from the federal government and are being probed by lawmakers over their high denial rates.
“It’s become a game of delay, deny and not pay,” Chris Van Gorder, president and CEO of San Diego-based Scripps Health, told Becker’s in September. “Providers are going to have to get out of full-risk capitation because it just doesn’t work — we’re the bottom of the food chain, and the food chain is not being fed.”
Scripps terminated MA contracts in January for its integrated medical groups, citing an annual loss of $75 million on its contracts with insurers.
In March, Bristol (Conn.) Health announced it was eliminating 60 positions, 21 of which are occupied and will result in layoffs. Its CEO, Kurt Barwis, laid blame on Medicare Advantage saying, “All the nice-to-haves are being taken out by the lack of insurance payment and the lack of reimbursement.”
In January, the Healthcare Financial Management Association released a survey of 135 health system CFOs, which found that 16% of systems are planning to stop accepting one or more MA plans in the next two years. Another 45% said they are considering the same but have not made a final decision. The report also found that 62% of CFOs believe collecting from MA is “significantly more difficult” than it was two years ago.
“Medicare Advantage net reimbursement right now is terrible for hospitals — our clients average about 85 cents on the dollar, and it’s only getting worse,” Mr. Ellsworth said. “MA is a race to the bottom, and I would argue that we’ve hit that bottom. Payers are going to struggle with this too, but no one wants to be the first to blink.”
Medicare Advantage denials increased almost 56% for the average hospital from January 2022 to July 2023, according to data from a joint American Hospital Association and Syntellis report. The denials and inconsistent reimbursement led to a 28% drop in hospital cash reserves.
Both Mr. Ellsworth and Mr. Kahn noted that it isn’t feasible for most health systems to completely walk away from Medicare Advantage, given that it now makes up more than half of the Medicare population. Instead, many hospitals are paring down contracts and looking for payer partners that align best with their financial objectives. Some systems are even exploring launching their own MA plan built in tandem with one insurer. Others have partnered with grocers or other health systems.
“We will ultimately pick a couple of partners going forward, and I think a lot of health systems are going to do this,” Will Bryant, CFO of Chapel Hill, N.C.-based UNC Health, told Becker’s in November. “They’re going to be the partners who act like partners and not who deny care in order to bolster their billions of dollars of quarterly earnings.”
Sachin Jain, MD, CEO of SCAN Group — one of the nation’s largest nonprofit Medicare Advantage companies — cautioned hospitals that dropping MA plans is a short-term trend that is “going to backfire in a big way for these large health systems.”
“You’re a nonprofit system saying you’re no longer going to accept the insurance that low-income people actually have,” he said. “We’ll see how that works out for you.”
Dr. Jain said any public policy program is going to create unintended consequences, adding, “What I would say to anybody who’s critical about the program is that you’re right, but let’s fix that.”
Former CMS Administrator Don Berwick, MD, toldBecker’s in February that the battle between hospitals and Medicare Advantage is a “manifestation of an underlying broken system in which everyone that gives care wants to give more, and everyone that pays for care wants to pay less.”
“To me, the untold story yet is about the physicians and nurses who don’t feel directly tied to ongoing Medicare Advantage trends, but they are certainly immersed in a changing financial landscape,” Dr. Berwick said. “As venture capital, private equity and ownership of healthcare by private interests increases, it changes their worlds, what it’s like to practice, their feelings about themselves, and the degrees of freedom they have to care for their patients. That chicken is going to come home to roost.”
Despite the tensions with hospitals, the MA program has bipartisan support in Congress and a 95% quality satisfaction rating among enrolled members in 2023. There are about 4,000 MA plans being offered this year nationwide, and MA members spend an average of $2,434 less on out-of-pocket costs and premiums per year compared to traditional Medicare enrollees.
“Medicare Advantage is very important, especially for low-income seniors,” Mr. Ellsworth said. “Hospitals need to acknowledge the reimbursement problem and proactively address their relationships [with payers] head-on.”
The fund covering Medicare‘s hospital-insurance benefits is now projected to run out of money in 2031, according to a new report by Medicare trustees.
This new insolvency date gives policymakers three more years than previously estimated to address impending financial setbacks that are facing the social safety net program, which provides health care benefits to tens of millions of Americans.
The ultimate insolvency date will likely change, the trustees say, due to difficulties in accurately projecting program expenditures. That leaves the exact timeline unclear for lawmakers to hash out a plan to mend Medicare’s finances, which could require an increase in taxes, a cut in benefits or a combination of both to keep benefits paying out in full.
What the report says
In a report released Friday, Medicare’s Board of Trustees provided the latest snapshot of the program’s finances. On the whole, Medicare is on sounder financial footing than indicated in last year’s trustee report, though financial shortfalls still loom.
Medicare hospital insurance benefits, aka Medicare Part A, are expected to fully pay out until 2031, a three-year improvement from the last trustee report.
Medicare Part B and Part D do not face insolvency, the report said, because they are funded separately — partially by premiums and general revenue from the U.S. Department of the Treasury. These benefits help cover typical health-insurance and prescription-drug expenses, respectively.
By contrast, Medicare Part A, which generally covers inpatient hospital care, skilled-nursing facility care, home-health care and hospice care, uses a separate reserve that’s funded by a 2.9% Medicare payroll tax. This is the trust fund at risk of insolvency.
In 2022, Medicare’s balance sheet looked better than previous years, the report shows. The hospital-insurance trust fund had a surplus of $54 billion, and Medicare overall brought in about $84 billion more than it paid out.
Nearly every year since 2008, the Part A trust fund has run a deficit, the report notes, with the exception of 2021 and 2022. The fund ran a steep shortfall in 2020 of more than $60 billion, largely because Medicare began making loans to health care providers to increase their cash flow as they grappled with the COVID-19 crisis. Then in 2021, providers began to repay Medicare, leading to the current surpluses.
The surpluses aren’t expected to last, however. Medicare trustees say the Part A program will begin running deficits again in 2025, drawing down the trust fund until it depletes in 2031. After that date, the program would not be bringing in enough money to fully pay out Part A benefits.
Key context
Medicare covered 65 million Americans last year. The vast majority of those people, about 88%, were 65 or older, though the program also provides health coverage to millions of disabled Americans.
Medicare — particularly Part A — has long faced financial issues. The nation’s changing demographic makeup is a big reason why. Because Medicare Part A relies on payroll taxes, it is more susceptible to insolvency when a growing share of the population is older, ultimately changing the worker-to-beneficiary ratio. In other words: less money coming in and more money going out. These demographic changes are also leading to insolvency issues for Social Security.
Compared to Social Security, projections for Medicare’s insolvency are less certain because it’s difficult for the trustees to accurately predict future health care expenditures. This can lead to some larger swings in the predicted insolvency date. By contrast to the trustee’s estimate, the Congressional Budget Office estimates the fund will remain solvent until 2033.
According to the nonprofit Center on Budget and Policy Priorities (CBPP), if Medicare Part A went insolvent, it would still be able to pay out almost all benefits. This leads some experts to call for tempered reactions to the newly projected insolvency date.
“Medicare does not face a financing ‘crisis’ and is not ‘bankrupt,’ as some critics charge,” tweeted Paul Van de Water, a senior fellow at the CBPP who specializes in Medicare. “Even if policymakers took no further action … tax revenues would still cover 89 percent of scheduled benefits” after the insolvency date.
Avoiding Medicare insolvency
Policymakers have several options to avoid impending insolvency headed for Medicare Part A. The trustees note two options that could immediately solve the issue:
The standard 2.9% payroll tax could be immediately raised to 3.52%, which would be enough to plug any financial shortfalls over the next 75 years.
In lieu of a tax increase, expenditures (read: benefits) would need to be reduced immediately by 13%, the trustees say.
Realistically, a combination of the two could work and the benefits cuts and/or tax increases could be implemented over a longer period of time.
Additionally, President Joe Biden released a plan last month to push the insolvency date back by 25 years.
The central change under the president’s plan would be a Medicare payroll tax increase on Americans earning more than $400,000.
Currently, earnings over $200,000 for individuals are taxed at 3.8% (while income under that amount is taxed at the standard 2.9% rate). These rates are split 50-50 between employees and employers.
The president’s plan introduces a new tier for income over $400,000, a tax rate of 5%.
The president’s Medicare proposal — part of a larger 2024 budget plan — is not expected to make it through the Republican-controlled House of Representatives.
Dozens of health systems ask CMS to crack down on Medicare Advantage Denials
Becker’s Hospital CFO Report
Rylee Wilson – Friday, March 22nd, 2024
Over 100 hospitals, health systems and providers signed on to a call for CMS to do more on Medicare Advantage denials.
Members of Premier, a healthcare services company, penned a letter to CMS administrator Chiquita Brooks-LaSure on March 21, requesting CMS collect more data on claims denied by Medicare Advantage plans and take enforcement action against plans not following the coverage rules set out by Medicare.
A survey of Premier’s member hospitals and health systems found 15% of claims to private payers are denied. A slightly higher portion of Medicare Advantage claims, 15.7%, are denied, according to the survey.
On average, hospitals spend $47.77 in administrative costs to appeal a denied Medicare Advantage claim, according to the Premier survey.
In the letter, the health systems asked CMS to monitor how much MA plans spent on direct patient care to address “potentially dire impacts on Medicare beneficiaries and providers.”
“It is imperative that CMS leverage its full authority to ensure that MA plans’ medical loss ratio (MLR) requirements for revenue used for patient care are satisfied in alignment with the benefits to which Medicare beneficiaries are entitled,” the providers wrote.
Dozens of health systems signed the letter, including CommonSpirit Health, Ascension, Advocate Health, AdventHealth and Providence.
The providers also asked CMS to bar MA plans from delaying or denying claims approved through electronic prior authorization and weight patient experience more heavily in its ratings of MA plans.
A growing number of hospital executives have criticized Medicare Advantage, often citing excessive prior authorization hurdles and delayed payments. A handful of systems have moved to drop the program entirely.
FEATURE ARTICLE 3
Nearly 15% of claims submitted to private payers are initially denied
Nearly 15% of medical claims submitted to private payers for reimbursement are initially denied, according to new survey data released Thursday.
Denied claims are more prevalent for high-cost treatments, with the average rejected charges at $14,000 and up, Premier Inc. reported. Medicare Advantage and other private payers eventually overturned more than half (54%) of denials, with the claims paid, but only after “multiple, costly rounds of provider appeals.”
The findings are from a national survey of hospitals, health systems and post-acute providers, conducted by the Charlotte-based healthcare improvement company.
“To address these potentially dire impacts on Medicare beneficiaries and providers, we urge CMS to stringently monitor MA plans’ reporting of expenditures on direct patient care,” Premier and 118 member organizations wrote in a March 21 letter to the head of the Centers for Medicare & Medicaid Services. “It is imperative that CMS leverage its full authority to ensure that MA plans’ medical loss ratio requirements for revenue used for patient care are satisfied in alignment with the benefits to which Medicare beneficiaries are entitled.”
Premier partnered with member hospitals to conduct the survey from October to December 2023. A total of 516 hospitals across 36 states, representing 52,123 acute care beds responded. Answers were based on claims submitted to private payers in 2022.
On average, hospitals and other providers incurred a cost of $43.84 per claim to fight denials. With insurers processing about 3 billion claims per year, this equates to $19.7 billion per year in expenses for these reviews. An average of about 3% of all claims denied included those that were already preapproved via prior authorization, Premier noted.
The continued burden from these delays and denials has impacted hospital finances. During the past year, average days of cash on hand at hospitals declined by 44 days or 17%. Meanwhile, days of cash on hand increased among insurers such as UnitedHealth Group (up 25.5% on average since 2019) and Cigna (24.4% on average).
The letter writers—who included numerous large health systems and other provider organizations—want CMS to take enforcement action against MA plans that “fail to abide by the coverage rules of Medicare.”
“Additionally, we note that CMS has moved away from holding MA plans accountable for [Consumer Assessment of Healthcare Providers and Systems] and other patient experience measures in recent rulemaking by reducing the weighting of patient experience and access measures in the Star Ratings program. We recommend that CMS return to its past policy of weighting patient experience and access measures more heavily in the MA Star Ratings methodology, empowering beneficiaries to hold their health plans financially accountable,” the letter stated.
The analysis does not specifically mention radiology services, but it mirrors ongoing problems imaging providers have had with prior authorization and the No Surprises Act (links to previous coverage below).
Ever since the passage of the Patient Protection and Affordable Care Act (ACA), commonly referred to as “Obamacare”, in 2010, the Department of Health and Human Services has dictated when and under what circumstances an individual and family can apply for and obtain health insurance. This period is known as the Open Enrollment Period, and it is upon us. Each year, between November 1st and December 15th, U.S. citizens and their families may apply for and obtain health insurance effective January 1st of the coming calendar year. From then until January 15th, they may apply for coverage effective February 1st. Beyond that date, they are locked out of any health insurance plan they were not enrolled in when the year ended. Only special circumstances such as losing “creditable” coverage through no fault of their own, moving out of a plan’s area, birth of a child, or death of a covered family member allow them to apply for coverage beyond the Open Enrollment Period. And only if they were insured when the special circumstance occurred and no more than 60 days have passed. Creditable coverage meets all the mandates of the Affordable Care Act, such as guaranteed coverage for pre-existing health conditions, including pregnancy and mental health disorders, along with no out-of-pocket for preventative medicine. All coverage is guaranteed so long as the above requirements are met.
If affordability of health insurance is an issue, Premium Tax Credits (subsidies) are available from the Department of Health and Human Services (DHS) to people or families whose income falls below a certain threshold.
WHO IS ELIGIBLE FOR THE PREMIUM TAX CREDIT?
To receive the premium tax credit for coverage starting in 2024, a Marketplace enrollee must meet the following criteria:
· Have a household income at least equal to the Federal Poverty Level (FPL), which for the 2024 benefit year will be determined based on 2023 poverty guidelines
· Can not have access to affordable coverage through an employer (including a family member’s employer)
· Can not be eligible for coverage through Medicare, Medicaid, the Children’s Health Insurance Program (CHIP)
· Have U.S. citizenship or proof of legal residency (Lawfully present immigrants whose household income is below 100 percent FPL can also be eligible for tax subsidies through the Marketplace if they meet all other eligibility requirements)
· If married, must file taxes jointly
Income: For the purposes of the premium tax credit, household income is defined as the Modified Adjusted Gross Income (MAGI) of the taxpayer, spouse, and dependents. The MAGI calculation includes income sources such as wages, salary, foreign income, interest, dividends, and Social Security.
Your tax credit is based on the household income estimate you put on your Marketplace application.
Income between 100% and 400% FPL: If your income is in this range (in all states) you qualify for premium tax credits that lower your monthly premium for a Marketplace health insurance plan. The lower your income is as a percent of the FPL—the higher your subsidy.
The easiest way to determine whether and for how much you qualify is to call me. You will estimate your 2024 household’s adjusted gross income and my subsidy calculator will tell us (based on the number of people in your household) how much your subsidy will be. If we give the DHS the same information you give me, my calculations are usually accurate to within $3.00 of what you will actually receive. We then apply that subsidy against the premium of the plan you wish to acquire and arrive at your net premium.
The number of people who qualify for subsidies continues to grow. For details on this, please refer to this chart and my feature article 2 below.
As to how much retail (gross) premiums are expected to grow from 2023 to 2024, estimates put the national average at 6%. (For the details on this, please refer to Feature Article 1 below.) Given the rate of core and real inflation, this should not come as a surprise. Acquisition of a subsidy will certainly offset ever-increasing premiums.
As always, the greatest challenge to the consumer and their agent/broker is affordability or obtaining the desired benefits. Instead, it is finding their doctors in the networks of a health plan. In 2024, as it was this year, there will be over 100 different plans available from six to eight different companies, depending on where one resides. Dealing with this myriad of options is where my three decades specializing in health insurance in the Houston area is invaluable. I know which hospitals are in which plan networks, and my provider search tools scan all plans without you having to go from company to company for results. Because I represent every company doing business in Texas, you can acquire information on all of them with one call to me.
Again, Open Enrollment begins November 1st, and for coverage during the entirety of 2024, it ends December 15th. Unlike going to the marketplace (Healthcare.gov) you will get me each time you call my local office with questions and for assistance and service–as opposed to an 800 number where you will get a different individual each time you call. My service is much more personalized and detailed than that of an hourly worker at the end of that toll-free number. If I don’t provide you with the level of service you deserve, I don’t have a client. And if I don’t have a client, I don’t earn a living. And it costs you no more to go through me than directly to the company whose policy you ultimately acquire.
I look forward to working with you and providing the best of service. Please call me.
D. Kenton Henry
Office: 281-367-6565 Text me 24/7 @ 713-907-7984 Email: Allplanhealthinsurance.com@gmail.com
This analysis of insurers’ preliminary rate filings shows that ACA Marketplace insurers are requesting a median premium increase of 6% for 2024. Insurers cite price increases for medical care and prescription drugs as a key driver of premium growth in 2024, In addition to inflation’s impact on medical costs, insurers point to growth in the utilization of health care, which fell in 2020 but has since returned to more normal levels.
Insurers’ proposed rate changes – most of which fall between 2% and 10% – may change during the review process. Although most Marketplace enrollees receive subsidies and are not expected to face these added costs, premium increases could result in higher federal spending on subsidies.
The analysis can be found on the Peterson-KFF Health System Tracker, an information hub dedicated to monitoring and assessing the performance of the U.S. health system.
Enhanced Marketplace subsidies have continued to drive up enrollment in the individual market, and the loss of Medicaid coverage by millions of people could contribute to this trend, according to a new KFF analysis. Meanwhile, enrollment in non-ACA-compliant plans is at a record low.
As of early 2023, an estimated 18.2 million people have individual market coverage, the highest since 2016. Individual market enrollment grew by about 29% between early 2020 and early 2023 — a result of enhanced subsidies introduced by the Inflation Reduction Act, increased outreach, and an extended enrollment period.
This enrollment growth could continue in 2023 as states resume Medicaid disenrollments amid the unwinding of the continuous enrollment provision. Some of the people losing Medicaid coverage may be eligible for subsidies on the ACA Marketplaces.
Due in part to the enhanced subsidies, about 4 in 5 individual market enrollees have subsidized coverage — the highest share since the ACA was implemented.
The number of people in non-compliant plans has fallen each year and could decrease further due to the Biden Administration’s proposed rule that would reverse the expansion of short-term plans. An estimated 1.2 million people were in non-ACA-compliant plans in mid-2022, compared to 5.7 million in mid-2015. These short-term plans often do not include certain benefits or coverage for pre-existing conditions and can impose a dollar limit on insurance coverage.
If unsubsidized premiums rise in 2024 due to higher health care prices and utilization, enhanced subsidies could shield most individual market enrollees from increases in their monthly payments.
























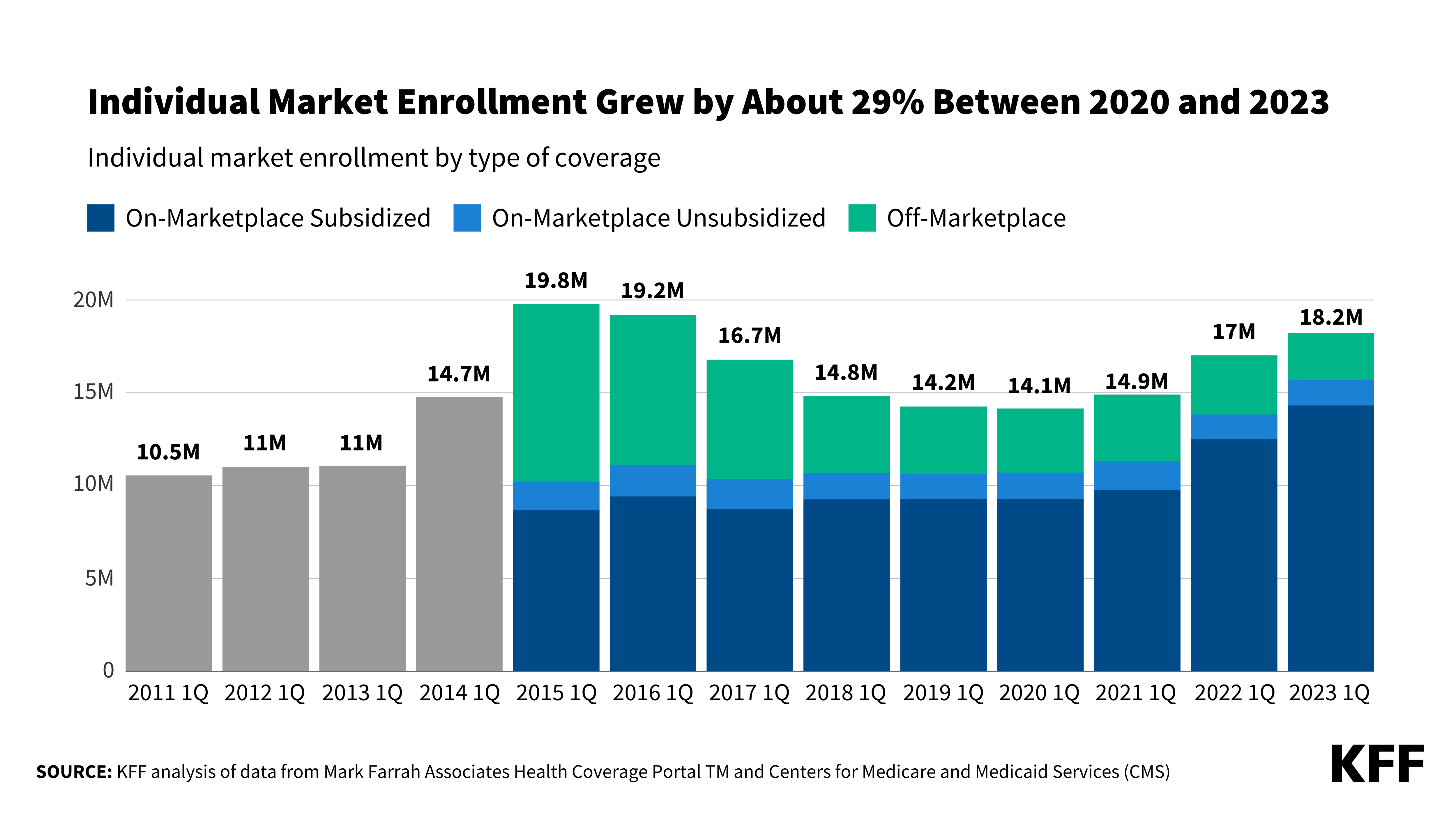{kind=link}
Leave a comment