
By D. Kenton Henry, editor
We are more than half-way through 2016 and three months away from the scheduled beginning of the 2017 Affordable Care Act (ACA) individual and family health insurance Open Enrollment Period (OEP). All of which finds this broker and many of his clients still reeling from the this year’s OEP which ended in February.
By last September, the rumor was health insurance premiums would not be inflating. That was quite encouraging to myself and to my clients who inquired as to such. However, what was unsaid―and to our shock―was what we learned with the commencement of OEP, November 1. Specifically, all carriers in southeast Texas (my major market) were eliminating Preferred Provider Organization (PPO) plans and forcing all new policyholders to accept Health Maintenance Organization (HMO) plans in their place. Anyone who knows anything about the latter knows that, with this type of plan, the patient must obtain treatment within the network or have no coverage whatsoever. For the young and bulletproof this seemed no great compromise. But to the middle-aged and older, whose health problems are moderate to very serious, it was a huge one. My existing PPO plan clients who were not grandfathered, including myself, were forced by the state’s largest insurance carrier (among others) to accept HMO coverage as a substitute or lose coverage altogether effective January 1, 2016. I scrambled to find acceptable replacement coverage for over 150 of my clients from the 2017 HMO plan options. This endeavor materialized into a “Mission Impossible” style nightmare as the HMO networks made available to them had nothing approaching the larger number of provider doctors and hospitals to which the employees and dependents of large employer plans had access. My clients learned they would be unable to utilize the providers in their current (and now former) PPO plans. It was mostly an exercise in futility attempting to find all of a person’s providers in any one network and, even if that person were so lucky, the inconvenience of getting their Primary Care Physician to refer them to a specialist was another cumbersome hurdle most considered an unwanted liability. After first enrolling in a higher cost Silver Plan offering doctor’s office copays, I myself, before the close of OEP, switched to a lower cost Bronze (non-copay plan) with another company. This after realizing it was virtually impossible for my physician to successfully maneuver the referral process. I made the decision it was best to take the premium savings involved in the benefit downgrade and have it for the occasional doctor’s visit which I have found to average $150. I save much more than this by having gone with a Bronze plan and―so far―it has worked out for me.
Since the close of OEP my phone rings throughout the week with people pleading with me to get them out of their HMO plan and into PPO coverage so they may see the doctor of their choice. I have only one PPO medical plan I can refer them to. This plan made itself available after the close of OEP but it is a hospital system plan which requires the patient remain in the system or face high out-of-network expenses. Furthermore, if the prospect has not had what the Department of Health and Human Services and ACA call a “Life Changing Event” they cannot change to a new plan at this time and must wait until October to enroll for a January 1 effective date. To add personal insult to injury, the plan does not even allow brokers and agents to be appointed with them for the purpose of doing business. Any business we refer or submit to them is done strictly on a “pro bono” basis. The only good news to be had for the consumer is that premiums not only stabilized but, in the case of those forced to migrate to HMO coverage, may have even gone down. Of course. Why shouldn’t they? The forced migration took client/patients from a position of having the final say on who their provider was to a position of having their providers, and therefore, treatment rationed. Most do not consider the trade off a worthy one. I know I do not. Of all my clients on individual and family PPO plans, forced to exchange such, some were small business owners. Those that had the minimum two W2 employees were able to switch to “Group” (employer based coverage) and maintain a PPO plan and provider network. If you fit this profile, please contact me. I can assist you in acquiring group coverage at any time throughout the calendar year.
My clients ask me if I expect PPO plans to re-enter the individual and family market in 2017. I tell them we will have to wait until the beginning of the OEP October 15th. But I advise them not to bet the ranch on it. If insurance companies do reintroduce PPOs, it will be only to entice policyholders to make a plan switch which would require a new contract (policy) in which brokers and agents would be excluded from compensation. This would be done in an effort to wipe the insurance companies books clean of the liability for our compensation. Their rationale is they can now put a great deal of the cost of enrolling people on the American taxpayer by directing prospective enrollees to the state and federal health insurance exchanges. The lion’s share will be directed to Healthcare.gov.
But what of the financial health and solvency of the insurance companies and their plans? Today’s feature article, from the New York Times (below) describes the push to ration provider access and treatment. Of course, they do not use those words, choosing instead to describe it as a move to “curb” cost in an effort to stabilize premiums. In spite of such, the insurers, for the most part, still struggle for solvency. The article explains that companies overestimated the number of ultimate enrollees and underestimated the cost of providing all the mandated care. To exacerbate their generally thin to negative profit margin, they did not receive all the government subsidies originally promised. Like so many programs, it would appear they cannot approach solvency without tax-payer funded subsidies.
Given all this, most of the insurance co-ops have failed and even major carriers are announcing withdrawal from the market. UnitedHealthcare, the nation’s largest health insurance carrier, has announced it will be pulling out of 90% of its current market in 2017. Anthem seeks to buy Cigna and Aetna seeks to merge with Humana. All this results in far less competition and . . . less competition means higher premiums for the consumer.
Stay tuned to see what the market offers us during this fall’s OEP. I will be focusing more and more on my “Medicare” clients who, much to my regret, were somewhat neglected during last fall’s scramble on my part to find new policies for 150 plus under-age 65 health insurance clients. Medicare recipients will be a priority this fall during their own OEP for Medicare Advantage and Part D Prescription Drug Plans. I hope the market allows me to play an active role in assisting families in obtaining health insurance. . . . We shall see. Predicting what is going to happen next in terms of what the general public refers to as “Obamacare” is a lot like walking into a swamp. You’re not quite certain if your next step will land in quicksand or on top of an alligator. Terra firma would be a welcome and unexpected change for the consumer and this agent / broker.
****************************************************************************************************
*FEATURED ARTICLE
New York Times
Business Day
Health Insurer Hoped to Disrupt the Industry, but Struggles in State Marketplaces
By REED ABELSON JUNE 19, 2016
Oscar Health was going to be a new kind of insurance company. Started in 2012, just in time to offer plans to people buying insurance under the new federal health care law, the business promised to use technology to push less costly care and more consumer-friendly coverage.
“We’re trying to build something that’s going to turn the industry on its head,” Joshua Kushner, one of the company’s founders, said in 2014, as Oscar began to enroll its first customers.
These days, though, Oscar is more of a case study in how brutally tough it is to keep a business above water in the state marketplaces created under the Affordable Care Act. And its struggles highlight a critical question about the act: Can insurance companies run a viable business in the individual market?
Oscar has attracted 135,000 customers, about half of them in New York State. And some of its efforts with technology have been successful. But for every dollar of premium Oscar collects in New York, the company is losing 15 cents. It lost $92 million in the state last year and another $39 million in the first three months of 2016.
“That’s not a sustainable position,” said Mario Schlosser, chief executive at Oscar.
Companies like Oscar were initially attracted by the potential of millions of new customers added to the individual market by the health law. But the reality has been far messier.
In an effort to attract customers, insurers put prices on their plans that have turned out to be too low to make a profit. The companies also assumed they could offer the same sort of plans as they do through employer-based coverage, including broad networks of doctors and hospitals.
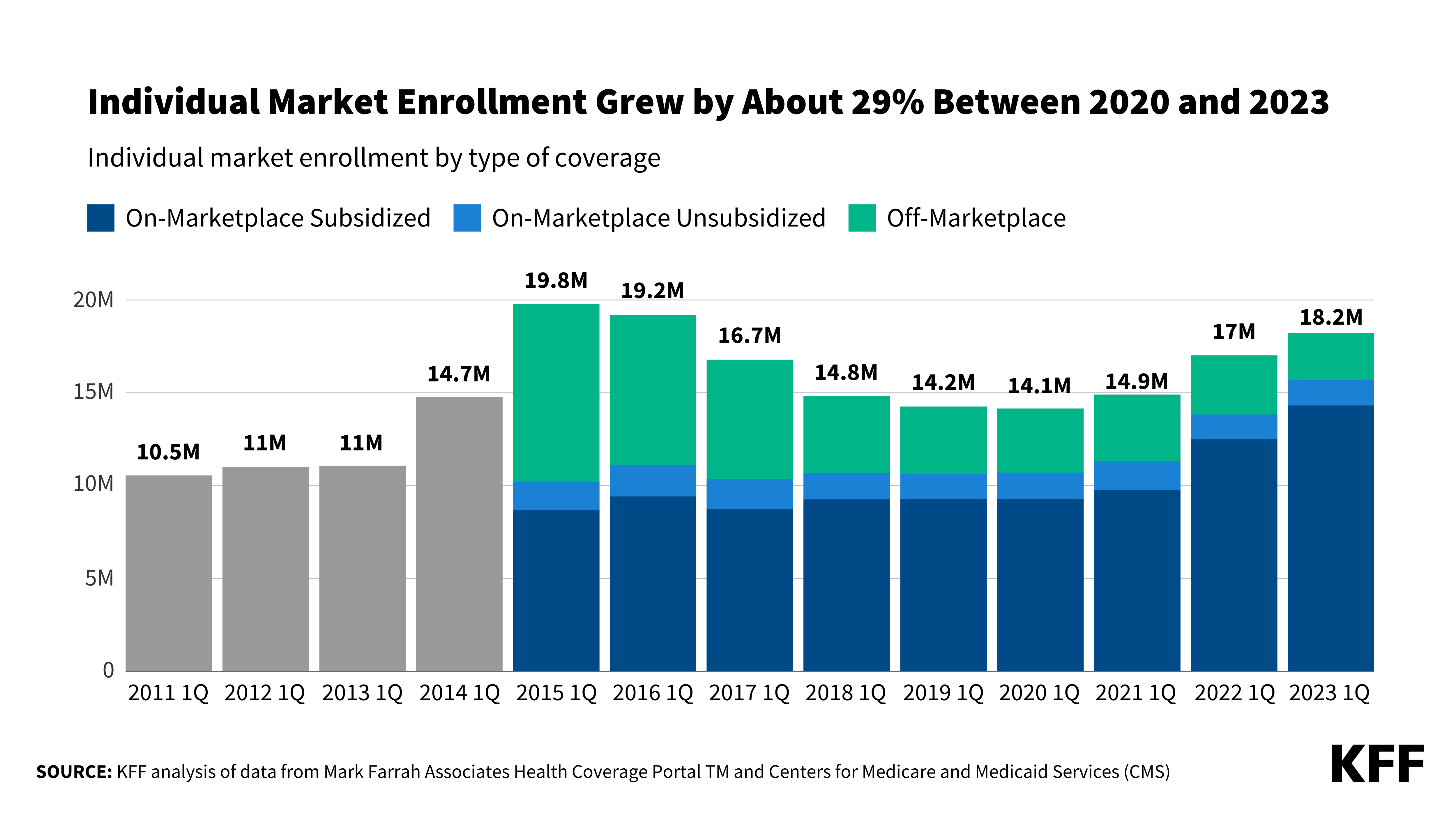
But the market has turned out to be smaller than they hoped, with 12 million signed up for coverage in 2016. Fewer employers have dropped health insurance than expected, for example, keeping many healthy adults out of the individual market.
And among the remaining population, the insurers cannot pick and choose their customers. The law forces them to insure people with pre-existing conditions, no matter how expensive those conditions may be.
As a result, most insurers are still trying to develop a successful business model. Last year, only a quarter of the insurers appear to have made money selling individual policies, according to a preliminary analysis from McKinsey, the consulting firm. Giant insurers like UnitedHealth Group have stopped offering individual coverage through the public exchanges in some states. And most of the new insurance co-ops, which were founded to create more competition, have failed.
A few times a week, Oscar Health serves a catered lunch for employees. The company has attracted 135,000 customers, but it is losing money. Credit Richard Perry/The New York Times
The heavy losses do not necessarily mean that the individual market is ready to implode. Some insurers, including large companies like Anthem, say they remain committed to the market, and some insurers have made money.
But the turbulence is certainly greater than expected. And it may well lead many insurers to seek double-digit percentage rate increases and tighten their networks.
“There was tremendous uncertainty that even the very established companies were flummoxed by,” said Larry Levitt, an executive with the Kaiser Family Foundation, which has been closely following the insurers’ progress.
Over all, insurance companies continue to make profits. The dearth of profits from the individual markets, though, show how challenging it is to make insurance affordable when it is not subsidized by the government or an employer.
The troubles in the individual market also underscore how some of the law’s provisions meant to protect the insurers have not worked as well as desired. Insurers did not receive all the payments they were due under one of the law’s provisions, and another provision, meant to even out the risk among companies to protect those that enroll sicker individuals, has been described as flawed by many health care experts. Federal officials have said they would tweak those formulas.
The companies that have fared best so far are those that have kept the tightest control over their costs, by working closely with low-cost providers or a limited group of hospitals and doctors. Many have abandoned the idea of offering the kind of access available through many employer plans. The successful companies have also avoided the very low prices found in some of the co-ops.
For most of the insurers, though, the math has just not added up, which is the case with Oscar.
In New York State, where Oscar is based, the company recently filed eye-catching requests to raise rates by a weighted average of nearly 20 percent for 2017. Regulators will make a decision in August.
“The market is over all too low in price,” Mr. Schlosser said. “We, like everybody else, have priced in a very aggressive way.”
Many of the big insurers, like Anthem, can rely on their other businesses to generate profits while they wait for this market to stabilize. Oscar does not have that luxury; it is focused on individual marketplaces. (In addition to New York, Oscar operates in California, New Jersey and Texas.)
Other new insurers that sell plans to employers or under government programs like Medicare have been a little more insulated. When Northwell Health, the system in New York previously known as North Shore-LIJ Health System, entered the insurance market, it created a new company. That company, CareConnect, has 100,000 customers, most of them individuals insured through both large and small employers.
“If we only had the individual market, we would have taken undue risk because we would not have understood that market,” said Alan J. Murray, CareConnect’s chief executive. He said the company is close to turning a profit.
Oscar says it plans to begin offering coverage to small businesses, but Mr. Schlosser was adamant that individuals will eventually be buying their own coverage, rather than relying on employers. The company is also racing to incorporate plans with smaller networks.
Bright Health, another start-up, also plans to work closely with health systems to offer consumer-friendly plans.
While Oscar has had to use another insurer’s network in New York, the company’s goal is to form partnerships with systems to create networks that specialize in managing care. The company began experimenting with these networks this year in Texas and California.
“Oscar talks about narrow networks like no one has seen one before,” said Dr. Sanjay B. Saxena, who works with insurers and health systems at the Boston Consulting Group.
Oscar has received $750 million from its investors, and Mr. Schlosser insists that the company understood how long it would take for the new insurance marketplaces to develop, calling these “very, very early days.”
Oscar points to its technological edge as a way to manage patients’ health better than the established insurers. It has created teams, including nurses, who are assigned to groups of patients and can intervene when its data flags a potentially worrisome condition like a high blood sugar level.
Promoting itself as a consumer-friendly alternative to the other insurers also has its risks. While Oscar has loyal customers, others say they are disappointed to find the insurer behaving like everyone else. Cosmin Bita, a real estate broker in New York, switched to Oscar from an insurer that had given him the runaround about whether it would pay for blood tests as part of his annual physical. Although Oscar said when he enrolled that the tests would be covered, he said, he found himself fighting with the company over whether everything was covered.
“The exact same thing happened,” Mr. Bita said.
Oscar executives said the company works hard to keep customers satisfied.
But so far, it has not proved that it has created a better model than the rest of the industry.
As Darren Walsh, a principal at Power & Walsh Insurance Advisors, said: “They haven’t invented a new mousetrap.”
http://healthandmedicareinsurance.com
















{kind=link}
Leave a comment