by D. Kenton Henry, Editor, Agent, Broker
The Open Enrollment Period (OEP) when individuals and families can select and enroll in health insurance plans for the calendar year 2018 is, just around the corner, beginning, as usual, November 1. What is different this year is, the Department of Health and Human Services (DHS), which oversees Obamacare (the Patient Protection and Affordable Care Act ― ACA), has proposed ending it December 15th ― a period half as long as in all previous years. OEP historically ends January 31st. If this proposed change is effected, consumers, and agents and brokers on their behalf, will be under considerably more pressure to bind coverage during a period which has always been fraught with confusion and frustration. Expected to heighten the latter, are increasing premiums and less participation by insurance companies and providers. Increasing premiums (which have only accelerated during Obamacare) speak for themselves. Less participation by insurance companies means less competition and fewer plans from which consumers may choose. Less participation by providers means it will be even harder to find your doctor or hospital in the Health Maintenance Network (HMO) plans we Texans are forced to choose from since January 2016. Do not expect Preferred Provider Organization (PPO) plans to return for 2018. The reason behind this deliberate trend is the unstated agenda of the industry to accustom each of us to have our providers―and thereby our treatment―rationed. The stated agenda is an attempt to mitigate financial losses by the insurance companies. Those in office who would replace Obamacare, and our current insurance system, with a “Single-Payer” system have no problem, whatsoever, with this trend. This, because restrictions on providers and treatment will be inherent in any single-payer program.There are many in Washington who believe the solution to healthcare insurance is to add all of us to Medicare.Those who share in the belief the single-payer system is the solution should consider the reality that Medicare is 50 trillion is debt and predicted to be insolvent 12 years from now. (That is according to the Trump administration. Obama’s predicted it to be insolvent one year earlier, the Congressional Budget Office three years earlier) http://www.modernhealthcare.com/article/20170713/NEWS/170719951
And this is the reality with current members having paid into it their entire working careers. How do you think that is going to work when you add every other American, a great many of which are not contributing to Medicare and never have? In my mind, that will expedite the path to insolvency exponentially. Consider a true single-payer program which serves as an example: Veteran’s Administration Health Care. A beacon of mismanagement resulting in waiting lines, provider rationing, and, in many parts of the country, long travel distances for care.
To exacerbate the difficulty in predicting premiums, and budgeting accordingly, President Trump has stated he is considering withholding federal subsidies to insurance companies. Historically, these have bought down the retail premiums the consumer must pay. Here we are halfway through September, and we still do not know if Trump will do so. Now―here is the real wrench in the grist mill ― the insurance companies must submit their 2018 premiums to the State Insurance Regulators by September 30th!
“If there’s no deal on the subsidies within the next five weeks, states will have no choice but to approve rate increases that include surcharges and go with those rates for the start of open enrollment on Nov. 1. On average that would mean consumers would see an extra 20 percent price hike next year.” ― 20 August 2017, CNBC.COM
“In many ways, the die has already been cast… if nothing changes before the end of September, we’re pretty much looking at those rates being locked in for 2018,” said Wisconsin insurance commissioner Ted Nickel, who is also president of the National Association of Insurance Commissioners. ― 20 August 2017, CNBC.COM
That is 20 percent on top of general premium increases predicted to be in the 12 to 15% range.
Once again, whether you feel you need assistance in coping with these issues in electing your 2018 coverage and protecting yourself and family from the sky-rocketing cost of health care, please call me at 281.367.6565. I have been specializing in health insurance for 26 of my 31 years in insurance. I have assisted my clients in coping with Obamacare since its passage in March of 2010.
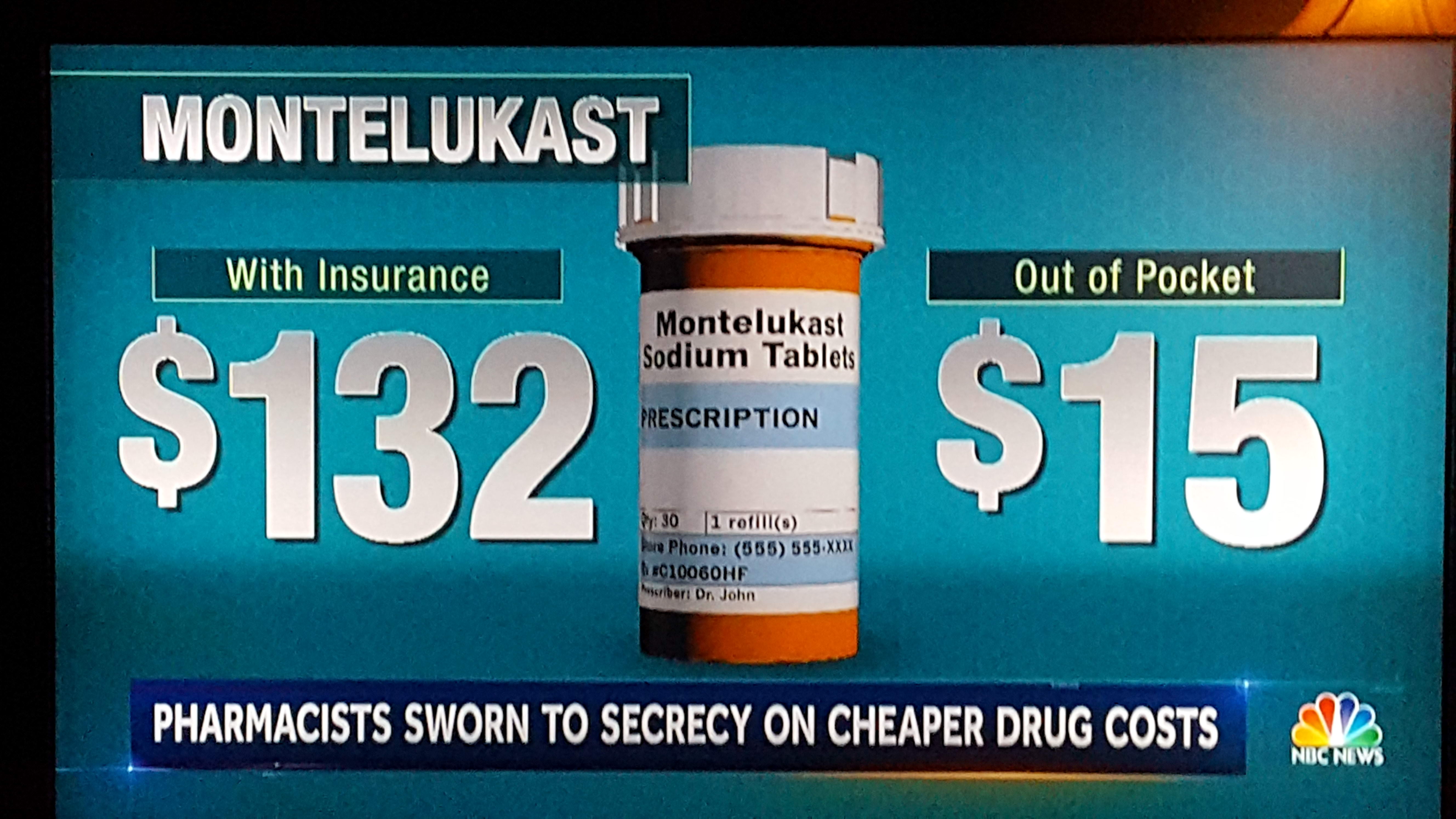
For those of you enrolled in Medicare ― Open Enrollment for election of your 2018 Part D Drug Plan begins, as usual, October 15th. Current clients should email me a list of your current drug regimen at allplanhealthinsurance.com@gmail.com. Upon receipt, I will provide you my recommendation your lowest out of pocket cost Part D plan in 2018. Those of you not currently my clients are encouraged to do the same.
http://thewoodlandstxhealthinsurance.com
https://healthandmedicareinsurance.com
*******************************
Featured articles:
Governors Tell Congress to Stabilize Individual Health Insurance Market
Michael Collins, USA TODAYPublished 1:25 p.m. ET Sept. 7, 2017 | Updated 5:45 p.m. ET Sept. 7, 2017
WASHINGTON — Governors from five states called Thursday on Congress to move quickly to stabilize the individual health insurance market and then embark on a serious effort to deal with skyrocketing health care costs.
“All of us — Republicans, Democrats and independents — should agree that our current path is not a sustainable one,” Tennessee Gov. Bill Haslam told a Senate panel.
The governors — three Republicans and two Democrats — testified during the second of four bipartisan hearings before the Senate Health, Education, Labor and Pensions Committee.
The panel is looking for a short-term fix to stabilize the individual market after the collapse of GOP efforts to repeal and replace the Affordable Care Act, or Obamacare.
The committee’s chairman, Sen. Lamar Alexander, R-Tenn., said he hopes senators can forge a bipartisan agreement by the end of next week and pass limited legislation by the end of the month to keep prices down and make it possible for everyone in the individual market to be able to afford insurance.
Congress must act quickly. New insurance rates for 2018 must be posted on the government’s website, healthcare.gov., by Sept. 27.
At Thursday’s hearing, the committee heard from Republican Govs. Haslam, Charlie Baker of Massachusetts and Gary Herbert of Utah and Democratic Govs. Steve Bullock of Montana and John Hickenlooper of Colorado.
A key issue is the future of federal cost-sharing payments to insurers that help them provide affordable coverage for low- and moderate-income families.
President Trump has threatened to end the payments, worth about $7 billion this year.
Read more:
With Obamacare in limbo, senators look for fix to stabilize health insurance market
Trump says GOP senators ‘look like fools’ on health care, warns of ‘imploding ObamaCare’
Congress has a crucial to-do list in September: Here’s what lawmakers must accomplish
All five governors testifying Thursday urged Congress to continue the payments, echoing the pleas of state insurance commissioners who appeared before the panel a day earlier.
The governors also called for creation of a reinsurance program that would limit losses to carriers that provide coverage in the marketplace and for the federal government to give states more flexibility to design and regulate insurance plans more suited to their own needs.
“It’s time for the federal government to work with us, not against us,” said Hickenlooper, arguing that state efforts to bring down premiums have been frequently undermined.
Without the federal government’s help, trying to keep insurance affordable is “like climbing one of Colorado’s famous 14,000-foot mountains in winter without crampons,” Hickenloopper said. “It can’t be done.”
Alexander said one option for giving states flexibility would be to allow the governor or state insurance commissioner to apply for a waiver from Obamacare’s rules, instead of waiting for the state legislature to act. He also suggested a “copycat” provision so that when one state wins federal approval for a program or initiative, other states could quickly follow suit.
Senators most likely will fashion a short-term stabilization plan that includes continuing cost-sharing for a limited period of time and gives states significantly more flexibility through Obamacare’s waiver process, Alexander said.
Once a short-term fix is enacted to stabilize the individual market, lawmakers can then move quickly to focus on how to make the market vibrant in the long run, Alexander said.
“I hope we can begin to spend most of our time on the larger issue of health care costs,” he said.
Two more hearings are planned next week. The committee will hear Tuesday from various health policy experts. Health care providers and other stakeholders will appear before the panel next Thursday.
Health Insurance
If Congress doesn’t fund Obamacare subsidies next month it could get pretty complicated
- Insurers can’t wait past a Sept. 30 deadline to set key insurance rates for next year.
- However, the fate of key subsidy payments under the Affordable Care Act is still unknown.
- State health insurance regulators expect that subsidies could remain in limbo past key deadlines, and are making plans for that possibility.
Bertha Coombs | @BerthaCoombs
Published 8:01 AM ET Sun, 20 Aug 2017 | Updated 4 Hours Ago CNBC.com
https://www.cnbc.com/2017/08/19/if-congress-doesnt-fund-obamacare-subsidies-it-could-get-complicated.html
State health insurance regulators have been hoping for the best when it comes to 2018 exchange enrollment, but are now bracing for the worst-case scenario — that the fate of key health insurance subsidies will remain in limbo past key deadlines next month.
“We have a way to protect consumers, but it is complicated and will cause unnecessary confusion and anxiety,” said Diana Dooley, chair of Covered California, the state’s Obamacare exchange, in a statement Friday.
California officials say they will wait until the end of September to decide whether to let insurers impose a 12.8 percent surcharge on 2018 exchange premiums to account for the potential loss of cost-reduction subsidies that reduce out-of-pocket costs for low-income enrollees.
“We are extending our deadline to give Congress time to act when they return in September,” Dooley explained. “We are heartened by the bipartisan discussion that put consumers first, but we can’t wait past Sept. 30.”
Some Republican lawmakers have proposed passing a short-term funding bill next month to authorize 2018 reimbursements for cost-reduction subsidies insurers are required to make under the Affordable Care Act.
However, if there’s no deal on the subsidies within the next five weeks, states will have no choice but to approve rate increases that include surcharges and go with those rates for the start of open enrollment on Nov. 1. On average that would mean consumers would see an extra 20 percent price hike next year.
“In many ways the die has already been cast… if nothing changes before the end of September, we’re pretty much looking at those rates being locked in for 2018,” said Wisconsin insurance commissioner Ted Nickel, who is also president of the National Association of Insurance Commissioners.
Pressure to act fast
State insurance commissioners, insurers and most of the major health industry groups have been urging Congressional leaders to fund the so-called cost-reduction subsidies for months, but politically it puts Republicans in a difficult spot after their failure to repeal the Affordable Care Act.
A federal judge ruled in favor of House Republicans last year, after they sued the Obama administration arguing that funding for the subsidies was never authorized by Congress. That lawsuit has been put on hold three times since last fall, and is due back in court this week.
President Donald Trump has repeatedly threatened to pull the plug on the insurer reimbursements citing the ruling, though the administration has continued to make the payments on a month-to-month basis, and will make them for August.
“What’s likely to happen is that Congress will pass some kind of interim funding, which negates the lawsuit,” said Julius Hobson, senior policy advisor at the Polsinelli law firm, adding that barring congressional authorization “it’s difficult to get a remedy that forces the government to spend the money.”
One thing that could help tip the balance for reaching a deal is the Congressional Budget Office’s report, which estimated that cutting the subsidies would increase the deficit by $194 billion over 10 years, in part because higher premium rates would result in more people qualifying for tax credits.
But Congress also has a number of key deals it has to reach next month, including raising the deficit and reaching an agreement to fund the government in order to avoid a shutdown.
What if the payments get funded after the rate hikes?
If funding for cost-reduction subsidies were approved after rates are locked in for open enrollment, consumers would not likely get relief from the price hikes right away.
“The Medical Loss Ratio that was instituted by the ACA will still be in place, meaning that consumers will be reimbursed [if] insures are not spending an 80% minimum on [health] care costs,” said Christina Cousart, senior policy associate at National Academy for State Health Policy, but she added those rebates would happen retroactively.
Some consumers might not be made whole for the premium surcharges. The higher rates would likely result in even fewer healthy unsubsidized consumers signing up for coverage. While the rate increases should be high enough to shield insurers from losses on sicker enrollees, they would not necessarily result in big rebates for consumers.
“There’s no way we can back out these higher rates that the companies put in… We’re going to have more expensive health insurance plans, we’re going to have fewer people enrolled,” said insurance industry consultant Robert Laszewski, president of Health Policy and Strategy associates.
What’s also unclear is whether consumers who receive larger tax credits would have to pay them back at tax time, if insurers do provide premium surcharge rebates.
“This is really hard to say at this point, without knowing how it will all play out — which is why we believe that the best solution is for Congress and the administration to resolve this issue now,” said Covered California spokesman James Scullary. “A resolution now eliminates the need for all of these workarounds to protect consumers.”
If Congress manages to come up with a funding deal to keep the subsidies in place, Wisconsin’s insurance commissioner says they should not stop there. He says the current problems underscore the need to give states more flexibility to stabilize their exchange markets than they have under current Obamacare rules.
“We have so little control now, so much of it is coming from the federal government through more of a central planning function rather than letting states engage in ways that best needs of their consumers,” said Nickel. “We do find ourselves in very difficult straights.”
*********************************
Changes Coming for Next Year’s Obamacare Open Enrollment Period
The Trump administration is working to make changes to the Affordable Care Act (ACA)
With the confirmation of Tom Price as Secretary of Health and Human Services, the Trump administration is already working to make changes to President Obama’s health reform law, the Affordable Care Act (ACA).
No, the promised “repeal and replace” of the ACA (also known as Obamacare) hasn’t happened yet, but Mr Price’s Department of Health and Human Services (DHS) has issued proposed guidelines that would affect consumers during 2018’s Obamacare open enrollment period.
The 2018 open enrollment period is not scheduled to begin until the fall of 2017. If the ACA is repealed, this next open enrollment period may be Obamacare’s last.
Let’s take a look at some of the proposed changes:
- Shorter open enrollment period for 2018 – The 2018 Obamacare open enrollment period is currently scheduled to run from November 1, 2017 through January 31, 2018. DHS’s proposed change cut the duration of the the open enrollment period by half so that it runs from November 1 through December 15, 2017.
- Some loosening of benefit requirements – The Obamacare law sets strict guidelines for “minimum essential coverage” that all major medical health insurance plans must provide. Though details are not yet available, DHS is proposing to loosen these rules somewhat, allowing insurers to offer plans with a broader range of coverage options.
- More supporting documentation required for special enrollment periods – Outside of the nationwide open enrollment period, consumers can only purchase coverage on their own when they experience a major life change, such as marriage or divorce, or the birth or adoption of a baby, etc. A proposed revision of rules would tighten the requirements for applicants to provide documentation proving their eligibility for a special enrollment period.
- Changes to doctor network rules – Under Obamacare, the federal government sets standards for what constitutes an adequate network of participating doctors and medical facilities for major medical plans. A proposed change from DHS would allow states to set these limits for themselves instead.
- Collection of overdue premiums – In a move designed to discourage applicants from neglecting to pay their monthly premiums near year’s end and simply re-enrolling with the same plan for January, a proposed DHS rule would allow insurers to collect overdue premiums before extending coverage to such applicants in the next year.
**************************************
Trustees’ report says Medicare will be insolvent by 2029
Modern Healthcare
By Virgil Dickson | July 13, 2017
The Medicare trust fund will be insolvent by 2029, the program’s trustees reported today.
The prediction is a year later than the 2028 date the Obama administration outlined in last year’s report. The Congressional Budget Office in January 2016 estimated the program would be solvent only until 2026.
Based on the new findings, the feared Independent Payment Advisory Board, which was designated by the Affordable Care Act to rein in Medicare costs if they grew faster than a set rate, will not be activated.
That’s likely good news as the board, called a death panel by ACA opponents, has never had to be formed. There hasn’t been the need, and some say, the willingness to expend the political capital. With midterm elections coming and possible fallout likely if Republicans repeal the ACA, this is one less possible political headache to worry about. Also of note, 2029 is 12 years longer than projected estimates before the Affordable Care Act become law.
However, trustees are worried doctors will exit the program anyway. The report contained new concerns about access to physicians in the coming years due to the Medicare Access and CHIP Reauthorization Act.
MACRA replaced the physician payment updates under the sustainable growth rate formula, which clinicians were paid under for years.
Under MACRA the annual physician payment update for 2017 through 2019 will be 0.5%. For 2020 through 2025, there will be no payment update, which alarmed the trustees.
“These amounts do not vary based on underlying economic conditions, nor are they expected to keep pace with the average rate of physician cost increases,” the report said. “Absent a change in the delivery system or level of update by subsequent legislation, access to Medicare-participating physicians may become a significant issue in the long term under current law.”
The new insolvency date does incorporate modest savings from the agency’s move to value-based care, including accountable care organizations. However, exact figures were not broken out.
“The innovations being tested under the ACA, such as bundled payments or accountable care organizations, could reduce incentives to adopt new cost-increasing technologies and could contribute to greater efforts to avoid services of limited or no value within the service bundle,” the report says.
Medicare Part D expenditures per enrollee are estimated to increase by an average of 6.4% annually over the next five years; that’s higher than the projected average annual rate of growth for the U.S. economy, which is 5.2 % during that period.
The report found that these costs are trending higher than previously predicted, particularly for specialty drugs.
In 2016, Medicare covered 56.8 million people and expenditures were $678.7 billion up from $647.6 billion and 55.3 million beneficiaries in 2015.
http://thewoodlandstxhealthinsurance.com
https://healthandmedicareinsurance.com